Preparation and features of the operation
Before performing a maxillary sinusotomy, the doctor will order a set of additional studies:
- blood test (general and biochemical);
- Analysis of urine;
- SASS-hemostasiogram;
- X-ray examination or CT scan of the paranasal sinuses;
- for patients of the older age group - ECG;
- if necessary, consult a therapist or neurologist.
Based on the laboratory data obtained, the doctor will decide on the possibility of carrying out the manipulation, since there are a number of contraindications - pronounced changes in the blood coagulation system, the patient’s severe somatic condition.
If the test results satisfy the doctor, then a date for the manipulation is set. The operation is carried out in the morning on an empty stomach, breakfast is prohibited, you can only drink.
There are three options for surgical access:
- through the frontal (front) wall;
- through the middle nasal meatus;
- through the oroantral anastomosis (fistula communication between the maxillary sinus and the oral cavity).
Depending on the choice of technique, type of surgical approach, extent and localization of pathological changes, and general condition of the patient, the surgeon chooses local anesthesia or anesthesia.
Classic technique of maxillary sinusotomy according to Caldwell Luke
Radical maxillary sinusotomy is performed both under general anesthesia and local anesthesia. Progress of the operation:
- Treating the surgical area with antiseptic substances.
- A horizontal linear incision of the gum tissue up to 6 cm wide is made under the upper lip.
- The tissue flap is separated and lifted up, thereby giving the surgeon access to the lower parts of the maxillary sinus.
- Using special instruments, a hole is created in the bone.
- The pathological contents (pus, foreign bodies) are scraped out and drained. The upper sections are treated carefully, since the wall between the maxillary sinus and the orbit is very thin.
- An artificial anastomosis is created with the nasal cavity, and a tampon is installed to remove the contents.
- Sutures are placed on the wound surface.
Radical maxillary sinusotomy is chosen when it is necessary to obtain wide access to the sinus cavity in severe, widespread pathological processes.
The disadvantage of this technique is the long recovery period and the high risk of postoperative complications (bleeding, damage to the trigeminal nerve).
Gentle endoscopic maxillary sinusotomy
Endoscopic maxillary sinusotomy is a popular technique today due to its less pronounced traumatic impact. Access is through a physiological opening - the nasal passage. The duration of the entire operation is no more than 30 minutes, the hospital stay is up to 3 days, but it can also be performed on an outpatient basis. It is performed under local anesthesia.
Sequence of manipulation:
- The surgical area is pre-treated with an anesthetic gel.
- The probe is passed through the nasal cavity at the level of the middle turbinate.
- If necessary, expand the passage by stretching or marginal excision.
- An endoscope consisting of a camera and a manipulator is placed into the maxillary cavity.
- After carrying out the necessary manipulations, they come out of the sinus.
Consequences of maxillary sinusotomy
The severity of the consequences of surgery depends on the treatment method. Microgaymorotomy and endoscopic surgery do not cause severe complications or consequences and do not require long-term postoperative recovery.
But after a radical maxillary sinusotomy, the patient requires long-term rehabilitation for 2-4 weeks under the supervision of a doctor. Classic maxillary sinusotomy can be complicated by damage to the trigeminal nerve, which may result in impaired facial expressions and the appearance of severe pain in the area of the nerve and its branches.
Classic maxillary sinusotomy can cause such dangerous consequences as:
- dysfunction of the trigeminal nerve;
- nose bleed;
- relapse of sinusitis;
- the formation of a fistula in the septum between the maxillary sinus and the oral cavity.
After the intervention, swelling and nasal congestion may persist for some time, and crusts and ichors may be discharged from the nose. Normally, swelling should disappear 7 days after the intervention. But in diseases of the vascular system and kidneys, tissue swelling persists for 10 days or more.
The following complications after maxillary sinusotomy may persist for 1-2 weeks:
- headache;
- nasal congestion;
- smell disorder;
- loss of skin sensitivity of the nose;
- numbness of lips;
- pain in the sinus, radiating to the ear and teeth;
- increased mucous discharge from the nasal cavity;
- temperature increase;
- facial deformation.
If the pain intensifies, nosebleeds or yellow mucus flows down the back of the throat, or body temperature rises, the patient should immediately make an appointment with a doctor.
Types of maxillary sinusotomy
There are classical (radical) maxillary sinusotomy and endoscopic maxillary sinusotomy.
Radical maxillary sinusotomy
The maxillary sinus operation is used to open the maxillary sinus through the mouth.
Radical maxillary sinusotomy is carried out using local or general (as indicated) anesthesia and includes the creation of access, excision of soft tissue, opening of the maxillary cavity and removal of polyps or foreign objects, formation of an anastomosis connecting the maxillary sinus with the lower nasal passage. The operation time is about an hour.
The essence of the operation
With an intraoral gairotomy, the otolaryngologist makes a horizontal incision in the soft tissues of the upper gum and moves them upward. Then, using special instruments, part of the bone plate on the facial wall of the maxillary sinus is removed. Thanks to the hole made, the sinus cavity becomes accessible for manipulation, and the otolaryngologist removes the pathological contents using a sharp spoon.
After scraping the mucous membrane, an anastomosis is formed with the nasal cavity, smoothing out the bone defect. A flap is made from the remaining free mucosa and placed on the bottom of the maxillary sinus to restore epithelization of its walls.
At the end of the operation, a tampon is placed in the sinus, which is removed into the nasal passage, and the wound on the side of the mouth is sutured. Using a tampon, sterility of the sinus is achieved and the accumulation of blood and pus is prevented.
After 48 hours, after preliminary anesthesia, the tampon is removed, and the patient is prescribed vasoconstrictor drops and sinus lavage. After a week, the sutures in the mouth are removed.
Endoscopic maxillary sinusotomy
Endoscopic maxillary sinusotomy is very popular as a minimally invasive and more gentle technique. With endoscopic maxillary sinusotomy, the lip is not dissected; the operation is performed through the nose. The procedure is virtually painless, characterized by minor swelling after surgery and does not leave scars.
What is endoscopic maxillary sinusotomy?
A gentle method is implemented in endoscopic maxillary sinus surgery - this is the elimination of mucus from the maxillary sinuses, which is not accompanied by an incision of soft tissues and the formation of scars. It is carried out using a special medical device - an endoscope, which also performs a diagnostic function. Observation of each manipulation is carried out using a microscopic video camera, which displays the image on a computer monitor.
Thanks to this, the surgeon evaluates every moment of the operation in a timely manner, and the doctors’ actions are clearly verified and accurate.
Using an endoscope, you can reach the maxillary sinus in five ways:
- through the middle passage of the nose;
- through the bottom passage;
- through a small depression called the “dog fossa” located on the upper jaw;
- through the dental alveolus;
- through the maxillary tubercle.
Based on the characteristics of the anatomical structure, the course of the disease and the presence of contraindications, in the case of each specific patient, the most convenient and effective method of access is selected.
Currently, endoscopic maxillary sinusotomy is being increasingly used; the course of the operation (see video in the section), which consists of punctures, expansion of physiological openings and suction of mucus, allows you to reduce tissue trauma to a minimum. The puncture diameter does not exceed 4 mm .
In addition, this technique causes less postoperative pain than the radical approach, and the rehabilitation time is almost halved. The advantages of this type of intervention also include the possibility of being carried out on an outpatient basis, since the manipulation time is no more than 30 minutes, and significantly reduced blood loss.
Thanks to a gentle technique, which includes endoscopic maxillary sinusotomy, the postoperative period is much faster and painless. Due to the fact that with this technique of influencing the maxillary sinus, healthy tissue is preserved, restoration of the mucous membranes takes less time. There are no external visible defects left, and with subsequent lesions of the nasal cavity, the air passage is no longer completely blocked, which will facilitate treatment in the future.
Using instruments with an endoscope, they not only eliminate inflammation in the maxillary and other sinuses, but also remove foreign objects that have entered the cavity.
Instruments for endoscopic examination of the nose
Features of rehabilitation
After a maxillary sinusotomy, the postoperative period may drag on for several months. This time will be needed for complete recovery. However, the most important processes occur in the first one and a half to two weeks. Usually the attending physician informs about all the features of rehabilitation, in particular, the patient needs to:
- Ensure yourself peace after the intervention, do not burden the body for one to two months. Physical activity is prohibited during this time.
- Take antibacterial drugs in the dosage prescribed by your doctor for a strictly defined course (usually five to seven days).
- If necessary, use anesthetics (medicines that relieve pain).
- Adhere to the rules of hygiene, in particular, the doctor may recommend rinsing the mouth with saline solution, etc.
- Visit your otolaryngologist regularly at the appointed time.
- Protect yourself from cold, overheating, and do not consume spicy or salty foods. You should also avoid fried foods and other frankly harmful foods. Alcohol is strictly prohibited. In general, you should lead as healthy a lifestyle as possible.
- Try to protect yourself from infections, avoid visiting places with crowds of people, etc.
Anesthesia
Surgery on the maxillary sinus is most often performed under local anesthesia. Infiltration and conduction anesthesia techniques are used. So, in addition to infiltration, infraorbital and tuberal, palatal and incisive anesthesia can be used. Modern painkillers are used - ultracaine, ubistezin, septanest.
Additionally, superficial anesthesia is performed in the area of the lower nasal passage.
In some cases, doctors resort to general anesthesia (endotracheal anesthesia).
Care after maxillary sinusotomy
Surgery requires the patient to stay in the hospital. How long it will take depends on the results of the operation and the body’s ability to recover. If the manipulation is successful and the prognosis is positive, the patient is discharged on the same day, with a subsequent three-day visit to the doctor at the ABC Clinic in Moscow. The otolaryngologist examines the nose and takes the necessary measures (rinsing and dressing). If we are talking about endoscopy in the area of the maxillary sinusotomy, then healing occurs quite quickly, without any special complications.
General wishes for the patient are quite common for all postoperative periods:
- Lack of significant physical activity.
- Antibacterial support (up to a week).
- Painkillers for pain.
- Rinse the nasal area with saline solutions.
- Vasoconstrictor drops or spray.
- General hygiene of the oral cavity and nose.
- Do not expose your body to high temperatures (sunlight, sauna, bathhouse).
- Avoid spicy and hot foods and alcohol.
- General strengthening of the body.
- Periodic examination by an ENT specialist.
Indications for maxillary sinusotomy
A maxillary sinusotomy is recommended if the patient is diagnosed with:
- chronic sinusitis (inflammation of the maxillary paranasal sinus);
- odontogenic sinusitis (inflammation of the paranasal sinus caused by disease of the tooth root of the upper jaw);
- the presence of a foreign body in the paranasal sinuses and paranasal passages;
- maxillary sinus cyst (a fluid-filled capsule is found in the maxillary sinus);
- polyp (a benign growth on the mucous lining of the maxillary sinus);
- trauma with damage to the walls of the paranasal sinuses;
- malignant or benign tumors of the maxillary sinus.
Surgical intervention is not performed in the following cases:
- bleeding disorders;
- exacerbation of chronic diseases;
- diseases, the course of which may be aggravated as a result of surgical intervention (systemic diseases of the respiratory system, hearing organs, oral cavity and jaw);
- impossibility of using general anesthesia (during pregnancy, lactation).
Possible complications
After a maxillary sinusotomy, complications arise, which are divided into physiological and pathological.
In the first case:
- the feeling of numbness of the lips caused by the action of the anesthetic substance disappears a few hours after the manipulation;
- swelling around the nose and mouth due to disruption of the integrity of soft tissues and vascular structures, which is leveled with the help of ice compresses;
- headache is a common consequence of any invasive manipulation and can be relieved with analgesics;
- a temporary increase in temperature, in the absence of surgical pathology, goes away without additional medicinal measures within a few days;
- pain in the upper jaw at the level of the teeth accompanies the postoperative period if access was made through the oroantral anastomosis;
- unpleasant sensations at the suture level during recovery from anesthesia.
The cause of the second group of complications is the addition of a bacterial infection, which requires immediate consultation with a doctor:
- pronounced unilateral swelling of the cheek at the level of the maxillary sinus;
- asymmetry of facial contours occurs when nerve structures are damaged during surgery;
- the release of a yellow mucous component signals infection.
Maxillary sinusotomy: when performed, types and course, consequences, rehabilitation
All materials on the site were prepared by specialists in the field of surgery, anatomy and specialized disciplines. All recommendations are indicative in nature and are not applicable without consulting a doctor.
Averina Olesya Valerievna, candidate of medical sciences, pathologist, teacher of the department of pathology. anatomy and pathological physiology, for Operation.Info ©
Maxillary sinus is an operation of opening the maxillary sinus in order to eliminate pathological contents from it (pus, granulations of the mucous membrane, foreign bodies, polyps).
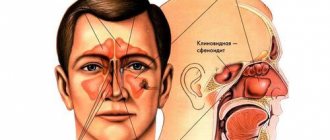
The maxillary sinus is a paired cavity in the upper jaw and is the largest paranasal sinus. It communicates with the nasal cavity through a small natural anastomosis, which opens into the middle nasal passage. The location of this anastomosis is such that drainage of the sinus in case of inflammation does not occur well enough.
Therefore, inflammation of the maxillary sinus (sinusitis) is the most common type of sinusitis, both acute and chronic.
Another feature of the maxillary sinus is that the roots of the teeth are located in its lower wall. The roots of 5-7 teeth can even protrude into the sinus cavity. When these teeth become diseased, the infection can penetrate into the sinus through the roots, so 10% of sinusitis are sinusitis of odontogenic nature.
Treatment of sinusitis
Sinusitis can be treated in several ways:
- Conservatively (antibiotics, vasoconstrictor drops, physiotherapy, nasal rinsing).
- Puncture of the maxillary sinus to extract pus and rinse.
- Surgical treatment (last resort) – maxillary sinusotomy.
When is maxillary sinusotomy indicated?
Maxillary sinus surgery is a last resort measure for treating maxillary sinus pathology. It is prescribed in cases where the disease cannot be cured by other measures. Mainly:
- Chronic sinusitis that does not respond to conservative treatment.
- Lack of effect from repeated sinus punctures.
- Odontogenic sinusitis.
- Polypous sinusitis.
- Cysts of the upper jaw.
- Neoplasms, suspected malignancy.
- Foreign bodies in the sinus (filling material, fragments of tooth roots, dental instruments).
- Complicated course of acute purulent sinusitis.
Maxillary sinusotomy can be classical or endoscopic.
Preparation for maxillary sinusotomy surgery
A maxillary sinusotomy operation is usually a planned operation (the exception is emergency maxillary sinusotomy for complications of purulent sinusitis - meningitis, orbital phlegmon).
Preparation for surgery includes:
- Computed tomography of the sinuses.
- X-ray of the sinuses.
- Maxillary sinusoscopy (not prescribed to everyone, according to indications).
- Blood and urine tests.
- Coagulogram.
- Microbiological culture of mucus discharge from the sinus.
- Fluorography.
- Examination by a therapist.
- Dentist examination.
- ECG for patients over 40 years old.
Contraindications for surgery
The operation will not be performed if there is:
- Acute infectious disease.
- Chronic diseases of the heart, lungs, liver, kidneys in severe cases.
- Decompensated course of diabetes mellitus.
- Blood clotting disorder.
- Exacerbation of inflammation in the sinus (relative contraindication).
Classic method of maxillary sinusotomy
This method is radical, since it provides the widest possible access to the sinus.
The operation is usually performed under general anesthesia; in rare cases, local anesthesia is possible.
The most common method of classical maxillary sinusotomy is the Caldwell-Luc maxillary sinusotomy.
Position – lying on your back. An incision is made in the oral cavity just below the transitional fold in the area of the projection of the anterior wall of the maxillary sinus, 4-5 cm long. The mucous membrane flap is moved upward.
Then a hole is made in the bone wall with a special drill or chisel. Use bone pliers to widen the hole. The diameter of the hole is about 1-1.5 cm. In this way, fairly wide access to the sinus is achieved.
maxillary sinusotomy according to Caldwell-Luc
The next stage of the operation is cleaning out the sinus with a special spoon. Pathological plaque, mucus, pus, granulations, and altered mucous membrane are removed. The sinus is washed with antiseptics.
Using the same bone instruments, partial destruction of the sinus wall is performed, separating it from the lower nasal passage. That is, a direct connection between the sinus and the nasal cavity is created. Iodoform turundas lubricated with Vaseline are inserted into this hole. They serve as drainage. The end of the tampon is inserted into the nasal passage.
The connection with the nasal cavity created during the operation serves for adequate drainage and aeration of the sinus, and through it the maxillary sinus can be washed with antibiotic solutions after surgery.
The wound on the side of the mouth is sutured.
The operation lasts about an hour.
After operation
Inpatient treatment after open maxillary sinus surgery is at least two weeks. After the operation, there is pain, discomfort in the face, swelling, numbness and impaired sense of smell.
Tampons are removed from the nasal cavity on the 3rd day. The sutures in the mouth are removed after a week.
After removing the tampons, the nasal cavity is washed with antiseptics, and vasoconstrictor drops are instilled. The sutures in the mouth are also treated daily, and rinses with an antiseptic are prescribed. To prevent infectious complications, broad-spectrum antibiotics are prescribed or taking into account bacterial culture of the discharge performed before surgery.
To reduce swelling of the face, it is possible to apply a pressure bandage to the cheek area, and applying ice is also practiced.
Cheek swelling may persist for up to 10 days. To speed up resorption, physiotherapeutic procedures (UHF, electrophoresis with drugs) are also prescribed.
The main advantages of open maxillary sinusotomy:
- Low cost.
- Can be performed in any ENT department.
- The greatest radicality of sinus sanitation.
Disadvantages and possible complications of classical maxillary sinusotomy:
- Traumaticity of the operation.
- Long period of hospitalization.
- A fairly long period of discomfort and inconvenience after surgery.
- High risk of complications (bleeding, damage to the trigeminal nerve, fistula formation).
The most severe complication after such a maxillary sinusotomy is damage to the trigeminal nerve. The consequences are impaired facial expressions, as well as severe pain in the area of the damaged nerve.
Basic recommendations after maxillary sinusotomy
To recover after surgery, follow these recommendations:
- Rest, limitation of physical activity.
- Taking antibacterial drugs for 5-7 days.
- Take painkillers as needed.
- Rinsing the nose with saline solutions.
- On the recommendation of a doctor, instillation of vasoconstrictor drops or sprays with glucocorticoids.
- Maintain careful oral hygiene.
- Avoid high temperatures (staying in the heat, baths, saunas, hot showers).
- Do not eat spicy, hot, too salty food or drink, and avoid alcohol.
- Avoid contracting a viral infection.
- Observation by an otolaryngologist within the specified time frame.
Patient selection
If the doctor suggests a maxillary sinusotomy, it means that most likely all other treatment methods no longer have any effect. Therefore, the operation should not be postponed. According to reviews from patients who have already undergone sinusotomy, this is still the most radical method of treating chronic sinusitis.
After the operation, constant nasal congestion, headaches, and discharge stop.
If there is a choice, it is better to choose endoscopic maxillary sinusotomy. In addition to all the advantages described above, with endoscopic surgery it is possible to simultaneously eliminate other problems that interfere with normal nasal breathing (correction of a crooked nasal septum, trimming of hypertrophied nasal turbinates, etc.).
The cost of radical maxillary sinusotomy starts from 10 thousand rubles (free surgery is possible). The cost of endoscopic maxillary sinusotomy is from 25 to 50 thousand rubles.
: report from the clinic about a sinusotomy
Source: https://operaciya.info/uhogorlonos/gajmorotomiya/
Other types of maxillary sinusotomy
Currently, there are many techniques for performing maxillary sinus maxillary sinus surgery, and all of them are widely used in otolaryngology.
The choice of one operation or another is made by the doctor, depending on the severity of the condition, the features of the facial structure and the ability of tissues to regenerate.
In addition to the classic Caldwell Luke maxillary sinusotomy operation, there are other methods:
- Moore's approach - characterized by penetration into the maxillary sinus through the external nasal cavity or an external incision along the nose.
- Denker approach - maxillary sinus maxillary sinus is performed in the same way as opening the maxillary sinus, as in the Luke technique.
- The Zimont operation - maxillary sinus maxillary sinus surgery is determined by extensive removal of the medial and anterior cavity of the maxillary sinus.
- Maxillary sinusotomy according to Zaslavsky-Neiman - is performed through opening the alveolus of the extracted tooth.
Postoperative rehabilitation
With radical maxillary sinusotomy, the patient remains in the hospital for 2–3 weeks. 3 days after the operation, the turundas are removed from the nose, and after 7 days the sutures in the oral cavity are removed. After 10 days, the swelling of the cheek goes away, and the patient is on the mend. Rehabilitation continues at home.
If there are no complications, there is no need for hospitalization after endoscopic maxillary sinusotomy.
Home rehabilitation can last up to 3 weeks. After a week, the swelling disappears, after 10 days breathing returns to normal. List of measures that are necessary to ensure that recovery after maxillary sinusotomy is quick and without complications:
- Eliminate physical and emotional stress.
- Do not visit the bathhouse or sauna.
- Don't take hot showers.
- Avoid eating spicy, salty, sour foods, alcohol, hot foods and drinks.
- Take systemic antibiotics for 5 to 7 days after surgery.
- Use vasoconstrictors, painkillers, and corticosteroids as recommended by your doctor.
- Rinse your nose with saline solutions 2-3 times a day for 7-14 days.
- Take a course of physiotherapy (electrophoresis, ultrasound and laser).
- Prevent colds and viral diseases.
Recovery period after surgery
The success of the procedure depends on the patient's recovery after it. After discharge from the hospital, the surgeon gives a referral to an ENT doctor to monitor the condition. You need to attend it for at least a month, and if necessary, the period can be extended. The doctor prescribes a course of antibiotics and solutions for rinsing the nasal cavity. At the same time, antihistamines and drugs to strengthen the vascular wall are added to the regimen if indicated.
After maxillary sinusotomy, slight swelling persists for a short period of time. Cinnabsin has a positive effect in this regard. It increases the body's own defenses and reduces swelling of the paranasal sinuses. Due to this, the patient's recovery after surgery is accelerated.
For a month, you should avoid visiting the pool and avoid eating spicy, cold or hot foods. Hypothermia should be avoided and preventive measures should be taken to avoid getting the flu or ARVI. After 1-2 months, it is advisable to visit a sanatorium or a course in salt caves for 10 days. The examination necessary to monitor surgical treatment is carried out 6 months after maxillary sinusotomy and 1 year.
Features of preparatory activities
Preparation measures include, first of all, establishing the absence of contraindications to the operation. Therefore, the doctor, before setting a date for its implementation, directs the patient to undergo tests:
- general blood and urine analysis;
- coagulograms;
- blood biochemistry.
In addition, the doctor will need the results of an X-ray examination of the sinuses and a computed tomography scan.
Since maxillary sinusotomy can only be performed with the use of anesthesia, you should stop taking liquids and food 6-8 hours before the start.
What types of operations are performed by doctors
Maxillary sinusotomy is differentiated according to several criteria:
- option for gaining access to the sinuses and technique (open, endoscopic, intranasal, and so on);
- the number of sinuses that are operated on (the organ is paired, that is, a person has 2 maxillary sinuses);
- with or without removal of cysts in the haumoral sinuses.
The final option for surgical intervention is determined by an otolaryngologist after consultation with a surgeon or traumatologist (depending on who will be assigned to perform the surgical intervention). A separate category includes “combined” maxillary sinus, when, for example, access to one sinus is obtained using a radical method, and to the second - using an endoscope. But such cases are extremely rare.
Classic - puncture
This type of classical surgical intervention is called a “puncture”. The purpose is to gain access to the internal volume of the maxillary sinuses in the nose, followed by pumping out the purulent contents and filling them with antiseptic solutions. Before the operation, the patient’s nasal cavity is cleared of mucus and other waste products, and vasoconstrictor drugs are instilled (to prevent excessive bleeding). The procedure itself involves inserting a Kulikovsky needle, with which a hole is made in the bone plate above the upper jaw (it is quite thin), after which the pus is pumped out using a sterile syringe, and then they are filled with an antiseptic solution.
Endoscopic (endonasal) maxillary sinusotomy with cyst removal
With this method, a small puncture is made, the walls of the sac are fixed, and then a thin endoscope tube is inserted into the sinus for subsequent intervention or visual examination of the cavity. Often the endonasal technique is used for maxillary sinusotomy with cyst removal.
Another option is to perform sinus clearance with endoscopic control. That is, when the doctor visually monitors the progress of the operation, if necessary, performs repeated drainage (if completely destroying the source of infection, one rinse with an antiseptic solution is not enough). Also, endoscopic control is mandatory when it comes to removing a malignant tumor.
Intranasal
The method involves performing an operation through the nasal cavity (maxillary sinusotomy can also be performed through the oral cavity, when the thin jaw bone is broken through). In the future, both an endoscope and a syringe needle can be applied to the maxillary sinus. During the procedure, only one side of the nasal cavity is involved; accordingly, the method is used if drainage of one sinus is necessary (for example, due to a hematoma or the presence of a cyst, tumor). It is considered a less traumatic method, with a shorter subsequent recovery period. This option can also be used if necessary to gain access to the ethmoid or frontal sinuses (complications of sinusitis). But despite its name, the procedure is not performed directly through the nostril, but through an incision or puncture from the supramandibular region.
Double-sided
That type of surgical intervention when the doctor gains access to two maxillary sinuses at once (the operation is often performed with a break of 1 to 2 days to monitor the patient’s condition). Two separate punctures are made (radical or minimally invasive method), each sinus is cleaned and treated separately. Most often, bilateral is used for chronic sinusitis, when simple rinsing does not give any effect or the inflammation has reached a stage where the outflow of mucus and pus is difficult. The likelihood of injury or subsequent complications directly depends on the instrument used by the doctor.
Radical
The main advantage of this method is extensive penetration, which allows the doctor to visually examine the condition of the sinuses and carry out high-quality cleaning, drainage, and treatment with antiseptic drugs. Quite often, a radical maxillary sinusotomy is performed if the need for its implementation arose against the background of massive dental inflammation (with suppuration of the tooth root and subradicular area, then the operation is performed through this hole, the remains of the damaged tooth and jawbone are first removed). The rehabilitation period is quite long, but the likelihood of developing any complications is extremely low.
Open maxillary sinusotomy according to Caldwell-Luc
It is not a minimally invasive method, but such an operation can be performed under local anesthesia. Currently, this type of surgical intervention is considered the most common due to the simple technique of its implementation and the absence of the need for expensive medical instruments. In this case, a part of the mucous membrane is initially removed and an incision is made in the soft tissues in the area of the upper jaw bone, which allows extensive access to the maxillary sinuses (performed through the oral cavity). The disadvantages of this type of Caldwell-Luc surgery are long-term rehabilitation, pain in the postoperative period (Analgin injections are prescribed), and there is a risk of damage to healthy tissue (in the first days after the procedure, the patient experiences discomfort when eating).
Microsinusrotomy
A general name for all endoscopic variations of maxillary sinus, regardless of how the doctor gains access to the maxillary sinuses (through the nasal, oral cavity, thin periosteum of the upper jaw, and so on) . The method can be used for diagnostic examination of the area of the maxillary or spongy sinuses (if a malignant neoplasm is suspected). Unfortunately, micromaxillary surgery is performed only in clinics with advanced technical equipment. A miniature camera is launched through the endoscope, while the doctor visually monitors the operation on the monitor screen.
Examination before maxillary sinusotomy
After the diagnosis is established and the need for surgical intervention is determined, the patient is prescribed the necessary tests. Laboratory and instrumental methods are used for this. The patient is sent for general blood tests, urine tests, biochemical studies, and blood coagulation is assessed. Instrumental images required for the operation are CT scans and radiography of the paranasal sinuses to assess their condition.
Surgery on the maxillary sinus: indications, preparation for surgery, how it goes - North-Eastern Administrative District of Moscow
Surgery on the maxillary sinus (maxillary sinus) is a rhinosurgical intervention performed for the purpose of sanitation, elimination of pathological contents and foreign bodies from the maxillary sinuses.
In addition to eliminating the inflammatory process, this operation is aimed at restoring full nasal breathing.
With a successful maxillary sinus surgery, the drainage function of the maxillary sinus anastomosis is completely restored.
Kinds
There are various methods of surgical intervention on the maxillary sinus:
- classic Caldwell-Luc operation (performed through an incision under the upper lip);
- endoscopic maxillary sinusotomy (performed via endonasal access, without incisions);
- minor surgical procedures (puncture of the maxillary sinus and its alternative - balloon sinuplasty using the YAMIK sinus catheter).
Indications
Factors and diseases that are direct indications for surgery:
- lack of effect from conservative methods of treating chronic sinusitis;
- maxillary sinus cysts (formations in the form of bubbles filled with liquid);
- the presence of polyps inside the sinus;
- the presence of neoplasms (if a malignant tumor is suspected, a biopsy is performed);
- foreign bodies of the maxillary sinus, which are a complication of dental interventions (fragments of tooth roots, particles of dental implants, particles of filling material);
- the presence of blood clots and granulations in the cavity;
- damage to the walls of the maxillary sinus.
The most common reason for surgery on the maxillary sinuses is sinusitis - inflammation of the mucous membrane of the maxillary sinus, which results in the accumulation of purulent exudate and the formation of hyperplastic changes in the mucous membrane.
Main symptoms
- nasal congestion;
- mucopurulent discharge;
- increased body temperature;
- symptoms of general intoxication of the body (weakness, drowsiness, malaise, headache);
- pain in the projection of the maxillary sinuses.
Preoperative preparation
Preparation for surgery on the maxillary sinuses includes a number of instrumental and laboratory studies. Before surgery you will need:
- computed tomography or radiography of the paranasal sinuses;
- rhinoscopy;
- general blood test (including leukocyte formula and platelet count);
- study of hemostatic function of the blood - coagulogram;
- general urine analysis;
- analysis for the presence of HIV, syphilis, markers of viral hepatitis;
- determination of blood group and Rh factor.
If the operation is planned to be performed under general anesthesia, it is additionally necessary to perform an electrocardiogram and consult with an anesthesiologist. It is very important to strictly follow the instructions given by this doctor, since their violation entails serious consequences.
Contraindications to maxillary sinusotomy:
- the presence of serious somatic pathology;
- blood clotting disorders (hemorrhagic diathesis, hemoblastosis);
- acute infectious diseases;
- exacerbation of chronic diseases;
- acute sinusitis (relative contraindication).
Minor operations: puncture and its alternative - balloon sinuplasty
The simplest surgical intervention on the maxillary sinus is a puncture (puncture), which is performed through the wall of the nasal passage for diagnostic or therapeutic purposes.
A more progressive method of restoring drainage of the maxillary sinus is balloon sinuplasty using a YAMIK catheter. The essence of this method is the atraumatic expansion of anastomoses by introducing and inflating a flexible catheter.
Next, a vacuum is created in the sinus cavity, this makes it possible to effectively remove the accumulated purulent exudate. The next step after cleansing is the introduction of a solution of medications into the sinus cavity.
This manipulation is performed under video control of endoscopic equipment, but can also be performed without it, which makes it accessible to most patients. The undeniable advantages of this method are:
- painlessness;
- no bleeding;
- maintaining the integrity of anatomical structures;
- minimal risk of complications;
- no need for hospital stay.
Endoscopic maxillary sinusotomy
This surgical intervention is performed through endonasal access, without violating the integrity of the wall of the maxillary sinus.
Modern endoscopic technology allows highly effective rhinosurgical procedures.
Thanks to the use of long-focus microscopes and high-quality fiber optic technology, high-quality visualization of the surgical field is achieved, which minimizes the risk of injury to healthy tissue.
The procedure for cleansing the sinuses is carried out using modern rhinosurgical equipment: a coagulator (performing the function of cauterizing tissues and blood vessels), a shaver (a tissue grinder with the function of instant suction), forceps and other surgical instruments. This is followed by rinsing with antiseptic solutions with the addition of broad-spectrum antibacterial drugs, proteolytic enzymes and corticosteroid hormones (in case of severe swelling).
Classic surgical method
The classic Caldwell-Luc procedure is performed via an intraoral approach. Most often, this method uses general anesthesia.
Main stages:
- Creation of access to the maxillary paranasal sinus by excision of soft tissue.
- Sanitation of the pathological focus (removal of polyps, granulations, sequestration, foreign bodies).
- Collection of material for histological examination.
- Formation of a complete communication between the maxillary sinus and the lower nasal passage.
- Installation of a drainage catheter for irrigation of the cavity with medicinal solutions.
Complications of radical maxillary sinusotomy:
- the possibility of developing intense bleeding;
- trigeminal nerve damage;
- fistula formation;
- pronounced swelling of the nasal mucosa;
- loss of sensitivity of the dentition and cheekbones due to surgical intervention;
- decreased sense of smell;
- sensations of heaviness and pain in the maxillary sinuses.
With minimally invasive interventions (endoscopic maxillary sinusotomy, puncture and balloon sinuplasty, complications occur quite rarely.
Postoperative period
There are a number of measures to reduce the risk of relapse of the disease and the occurrence of various complications:
- irrigation of the nasal cavity with water-salt solutions;
- desensitizing therapy (taking antihistamines);
- local use of topical corticosteroids;
- antibacterial therapy;
- taking medications that strengthen the walls of blood vessels.
As a rule, the postoperative rehabilitation period lasts about one month. It is not advisable at this time
- eating hot, cold, spicy foods;
- perform heavy physical work (especially related to heavy lifting);
- visiting baths and saunas, swimming in the pool.
You should also avoid hypothermia and contact with ARVI patients. A good end to the rehabilitation period would be a sanatorium treatment at a seaside resort or a visit to a salt cave. Within a year after surgery, you should be observed by an otolaryngologist.
Source: https://www.polyclin.ru/operaciya-na-gaymorovoy-pazuhe/
How is the endoscopic procedure performed?
The course of the operation in this case is somewhat different from the technique of classical maxillary sinusotomy.
The instruments used in the process are inserted into the sinuses through the nose, mouth, or small punctures in the tissue. Small and medium degrees of damage to the patient allow operations to be performed using the endoscopic method.
The manipulations do not require the use of general anesthesia - before starting, the patient is given local anesthesia.
The doctor uses a special endoscope - a hollow elastic tube, which is equipped with optics, illumination and a camera. In addition to the fact that the endoscope gives the surgeon a picture of the operated area, displaying it on the monitor, medical instruments can be inserted through the cavity of the tube to carry out all the necessary surgical actions.
Endonasal maxillary sinusotomy lasts no more than 20-30 minutes. During this time, the doctor examines and cleans the sinus cavity, removes cysts and tumors, and rinses the cavity with a disinfectant solution.
To improve the natural outflow of fluid from the sinus, a balloon sinus rhinostomy can be performed - expansion of the anastomosis of the maxillary sinus. Punctures made to insert instruments do not always require sutures. The patient remains in the hospital for 2-3 days after surgery.
Rehabilitation in this case takes about 2-3 weeks. Complete tissue restoration will take no more than a month. During this period, it is recommended to limit physical activity so as not to provoke bleeding.
The patient needs to periodically measure his temperature after surgery, as well as monitor his own sensations. If the pain that occurs after the intervention is quite severe, you should take non-steroidal anti-inflammatory drugs such as ibuprofen or paracetamol. They usually go away after a few days. If bleeding from the nose is added to the pain, you should immediately consult a doctor.
How long does swelling last after surgery? In most cases, it begins to decrease after two or three days. After a week, swelling of the nose and nasal passages should disappear, and nasal breathing should be restored.
It should be noted that endonasal maxillary sinusotomy, although it takes place with less intervention in the tissue, can also cause complications in the form of bleeding, re-formation of sinusitis or fistula.
Judging by patient reviews, minimally invasive endoscopic surgery, although more expensive than radical surgery, is more preferable than the classic type of intervention. It is faster, easier to tolerate and does not require a long stay in a hospital.
On average, healing of the mucous membranes and the patient’s return to normal condition takes up to a month after endoscopic maxillary sinusotomy, and up to two months if a radical procedure was performed.
Sinusotomy, carried out in compliance with all the rules of asepsis and surgery, allows you to get rid of sinusitis, swelling and neoplasms of the mucous membrane with a high probability. In the process of penetrating the sinus cavity, the doctor is able to remove pathological contents, blood clots, remains of dental roots, fillings, and any foreign bodies.
Some patients note that after a while there is a relapse of sinusitis, which is why the operation has to be repeated. On average, relapse of the disease occurs in 20-30% of cases.
Source: FoodandHealth.ru
Indications and contraindications for surgery
Sinusitis is the most common type of sinusitis. Most often it occurs as a complication of a respiratory infection. Often the cause of sinusitis is pathologies occurring in the periapical tissues of the upper teeth.
Inflammatory diseases in the maxillary cavities are treated in different ways. In the uncomplicated course of such diseases, antibiotics, nasal drops, nasal lavage and physiotherapy are used.
In more severe cases, they resort to puncture of the maxillary sinuses to remove purulent contents and rinse. Sinusotomy is the most radical treatment for sinusitis, used when other methods do not bring results.
Indications for maxillary sinusotomy are the following pathologies:
- chronic sinusitis, if conservative therapy is ineffective;
- purulent sinusitis, occurring in an acute form, with complications (a purulent process is indicated by the appearance of an unpleasant odor from the nose);
- sinusitis of odontogenic etiology (infection penetrates into the sinus of the upper jaw from the roots of the upper teeth);
- tumor processes of various types;
- sinus cysts;
- detection of a foreign body in the maxillary sinus (a tooth fragment, filling material that penetrated into the sinus through a tooth socket, particles of synthetic materials after intraosseous implantations);
- nasal polyps;
- blood clots;
- damaged walls of the maxillary sinuses.
Sometimes surgical interventions on the maxillary sinuses cannot be performed. A relative contraindication is exacerbation of a chronic inflammatory process in the sinuses. It is necessary to first relieve acute symptoms, except in cases where an acute purulent process develops, threatening dangerous complications (the development of meningitis, sepsis, periostitis). Then the operation is undertaken in the acute period to prevent aggravation of the patient’s condition.
Surgery is not performed for the following diseases:
- acute infections, aggravated chronic diseases;
- severe cardiovascular and pulmonary pathologies in the stage of decompensation;
- insufficiency of liver and kidney function;
- decompensated diabetes mellitus;
- diseases accompanied by blood clotting disorders.
Patients carrying a child are recommended to choose gentle methods of maxillary sinusotomy that do not require general anesthesia.