“Bronchi cancer” is a term that is rarely used by doctors. In medicine, the more common concept is “bronchopulmonary cancer,” which combines malignant tumors of the lungs and bronchi. This approach to terminology arose due to the fact that the lung tissue and the bronchial tree are closely related, both in an anatomical and functional sense.
Some figures and facts regarding bronchial cancer:
- The disease most often occurs in older people. In more than half of cases, bronchial cancer is diagnosed after the age of 50 years. Another 25% of cases occur in the age group of 40–50 years.
- The main cause of malignant tumors of the bronchi is smoking. Up to 80% of patients are smokers.
- Most often, the tumor occurs in the upper parts of the bronchial tree, since they are better ventilated, and carcinogens contained in the inhaled air are more likely to lead to malignant transformation of cells.
Structure of the bronchial tree. In which bronchi do malignant tumors occur?
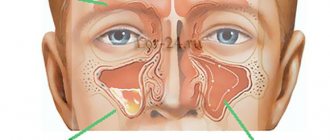
The air that a person inhales passes through the nose, pharynx, larynx, and trachea. At the level of the upper edge of the fifth thoracic vertebra, the trachea ends and divides into two main bronchi . This location is called the tracheal bifurcation . The main bronchi are the first order bronchi , they are divided into lobar (second order) , then into segmental (third order), subsegmental (fourth order), lobular, and finally into terminal (end) bronchioles.
All these branches together make up the bronchial tree . The walls of large and small bronchi are structured in the same way: on the inside they are lined with mucous membrane , under it there is a framework - fibrocartilaginous membrane , on the outside - the adventitial membrane.
Malignant tumors that originate from the mucous membrane are called cancer. They can occur in any part of the lung, but are most often found in the hilum - where the main bronchus enters the lung. In two thirds of cases, cancer develops in the bronchi of the first, second and third order.
Diagnostics
The disease should be diagnosed by a pulmonologist or therapist, so when the first signs of pneumonitis appear, you should consult a doctor.
After clarifying the patient’s complaints, the medical history and the presence of occupational hazards must be studied in detail. The patient notes the presence of frequent pneumonia with an atypical course. Next, a physical examination is performed. The doctor may detect increased breathing, cyanosis of the nasolabial area, and changes in the fingers and nails characteristic of chronic pulmonary heart disease. With shortness of breath, there is retraction of the pliable places of the chest during inspiration (intercostal spaces, jugular fossa) and swelling of the wings of the nose. On auscultation, harsh breathing and moist medium-caliber rales on inspiration may be heard.
Instrumental diagnostic methods include X-ray examination of the lungs in two projections, computed tomography or MRI. Various changes in the pulmonary fields are detected: infiltrative, ground-glass opacities, increased pulmonary pattern and its deformation, “honeycomb lung” pattern.
It is necessary to assess the function of external respiration using spirography, which reveals different types of disorders: obstruction, restriction or mixed. Additionally, bronchoscopy and bronchography can be performed. During bronchoscopy, bronchoalveolar lavage can be performed, followed by analysis of the lavage water. A lung biopsy may be needed to definitively confirm the diagnosis.
A blood test for hypersensitivity pneumonitis reveals an increased number of eosinophils, which indicates the allergic nature of the disease. There will also be changes in the blood characteristic of the inflammatory process: an increase in ESR, leukocytosis. In case of respiratory failure, a blood gas analysis is prescribed. Microscopy and bacteriological culture of sputum are required, primarily to exclude tuberculosis.
Classification of bronchial cancer
The histological (based on the appearance of tumor cells under a microscope) classification of bronchopulmonary cancer includes four main types of tumors:
- Small cell cancer occurs mainly in smokers, is highly aggressive, spreads quickly and is difficult to treat. It accounts for about 12% of all cases of bronchopulmonary cancer.
- Squamous cell carcinoma , together with the next two types, combines into a group of non-small cell tumors , which account for more than 80% of all cases of lung cancer. The risk of developing squamous cell carcinoma is strongly associated with smoking.
- Adenocarcinoma is most common among women and nonsmokers. Unlike squamous cell carcinomas, adenocarcinomas are usually smaller in size and tend to grow in the peripheral parts of the lung. A separate subgroup of bronchoalveolar adenocarcinomas is distinguished.
- Large cell carcinoma consists of large, undifferentiated cells.
Depending on how much the tumor tissue has lost its normal features, poorly differentiated and highly differentiated tumors are distinguished. The first ones are more aggressive.
When choosing treatment, the location of the tumor foci is of great importance. Depending on this indicator, bronchopulmonary cancer is divided into two types:
- Central - the tumor is located in the bronchi of the 1st–3rd order (main lobar, segmental).
- Peripheral - the tumor is located in the smaller bronchi.
Lungs' cancer
Oncological tumors in the lungs can affect the central parts of the organ, peripheral tissues, or the tumor spreads in a mixed type. Central cancer grows in the area of small and large bronchi. This form of pathology occurs most often. The tumor grows into the thickness of the lung tissue, disrupting the normal functioning of the organ.
Clinical symptoms of central (squamous cell) cancer of the initial stage:
- dry cough;
- bronchitis or pneumonia that is difficult to treat;
- pain in the chest area of varying intensity;
- difficulty breathing, shortness of breath after physical activity;
- wheezing, hoarseness of voice;
- yellow or gray skin tone;
- inflammation of peripheral lymph nodes;
- depression, apathy;
- sudden weight loss.
Hoarseness in the voice can occur with paralysis of the vocal cords and muscles. At first, during a cough, no sputum is produced, then a purulent exudate appears, often mixed with blood. As the disease progresses, the tumor grows into nearby organs with subsequent disruption of their functioning.
Paracancrosis pneumonia or pneumonitis, which develops against the background of an oncological neoplasm, is difficult to treat, but noticeable improvements are observed after taking antibiotics. The patency of the bronchi can be restored, and the inflammatory process is reduced. This is why diagnosing the pathology is difficult.
Peripheral cancer in the initial stages is asymptomatic.
Damage to the lung tissue is observed more often in the upper sections. After the tumor increases in size, characteristic signs appear; usually such disorders are detected in severe forms of the pathology, when metastasis has occurred.
It is important to promptly detect lung cancer at an early stage. In such cases, surgical treatment is performed and courses of chemotherapy are prescribed. These methods allow a person to be cured in 80% of cases.
Stages of bronchial cancer
Bronchopulmonary cancer is divided into stages depending on how far the tumor has spread in the body. In this case, they are guided by the generally accepted TNM classification. The letters in it mean:
- T—size of the primary lesion, degree of invasion into adjacent tissues.
- N - damage to regional (close to the primary tumor) lymph nodes.
- M—presence of distant metastases.
Depending on these indicators, the stage of the tumor is determined, which is designated by Roman numerals I–IV.
Characteristics of types of cough in pulmonary oncology
Bronchogenic cough varies depending on the stage of development of carcinoma and the severity of the pathology. The clinical picture of lung carcinoma includes 5 types of coughing attacks:
- Short. It is caused by a strong contraction of the abdominal muscles and often appears at the first stage of development of a malignant neoplasm. With a short cough, a powerful release of air occurs due to the reduction of the trachea.
- Strong. It is permanent and intensifies at night. It is accompanied by muscle spasms of the respiratory tract. Severe coughing attacks often result in vomiting, and in severe cases, cardiac arrhythmias and loss of consciousness.
- Dry. A dry cough is characterized by the absence of sputum, tearfulness and debilitation. It provokes the development of pain and indicates significant damage to the pulmonary structure. The attacks can be silent, barking, muffled and hoarse.
- Wet. It most often occurs in the morning and at night and is characterized by copious discharge of sputum and mucus, ranging in color from yellowish to brown. This cough characterizes damage to the bronchial structure.
- Hemoptysis. Indicates severe damage to large pulmonary vessels, as well as increased pressure in the chest. It is permanent in nature with the release of sputum of a bright scarlet color. Accompanied by respiratory failure, severe pain and a feeling of heaviness in the chest.
Note! If the discharge of sputum with blood and coughing attacks due to lung cancer suddenly stop, this may indicate toxic damage to the body by metabolic products of the cancer tumor!
If lung cancer is diagnosed in time, this will significantly increase the patient’s chances of life. Therefore, when the first coughing attacks occur, you need to consult a doctor and also undergo a fluorographic examination.
Symptoms of bronchial cancer
In the early stages, there are most often no symptoms. The tumor is diagnosed accidentally during an x-ray. Regular fluorography helps in early diagnosis. Experts from the American Cancer Society recommend that long-term smokers consider regular CT scans. Such periodic studies designed to diagnose cancer in early, asymptomatic stages are called screening .
Possible symptoms of bronchopulmonary cancer:
- Persistent chronic cough.
- Sputum mixed with blood.
- Dyspnea.
- Chest pain.
Even when symptoms appear, it is not always possible to recognize a malignant tumor immediately. The picture may resemble sluggish pneumonia, pleurisy, or another disease. It is important to be attentive to your health. If you experience any unusual symptoms, if they persist long enough, you should contact your doctor and get tested.
Book a consultation 24 hours a day
What is paraneoplastic syndrome in bronchopulmonary cancer?
Cancer cells produce various substances that enter the bloodstream and can cause pathological changes in the body. This leads to the so-called paraneoplastic syndrome . In lung and bronchial cancer, the tumor often affects the nervous system. This manifests itself in the form of disturbances in gait, balance, coordination of movements, swallowing, speech, memory, vision, sleep, etc.
Characteristics of cough types in lung cancer
The pathological process, that is, chronic cough, can be characterized as:
- rare/frequent;
- strong/weak;
- short/long;
- raucous/loud;
- jerky/rolling;
- painless/painful;
- wet/dry.
For a cancer tumor that is based in the body of the lung, the following types of cough are not typical: strong, short and loud. Patients who make similar sounds when coughing most likely are not carriers of lung cancer; their larynx and trachea are susceptible to infectious diseases, and in rare cases, the tumor is localized in these organs and not in the lungs. If such changes are not recognized in time and treatment is prescribed in accordance with oncological protocols, you can skip the intensive cycle of disease development and allow it to enter the subacute stage, which will certainly end in death.
Characteristic cough intonations when irritating receptors located in the lung tissues:
- Lengthy, muffled, weak and deep - indicates a sharp decrease in the elasticity of the lung tissue, as well as the presence of one or more pathological foci in this organ. Treatment should be symptomatic.
- Pain in lung cancer, characteristic of constant coughing, tells the specialist that the tumor has affected the pleura around the lungs or is localized in the bronchi, which are sensitive to pain impulses. The pain may intensify with intense movement of the sternum. In the case when auscultation gives the result in the form of a painful cough and bursting noises, this means only one thing, fluid begins to accumulate between the pleura and the lung.
- There are two types of wet cough: with regular release of liquid contents and with expectoration of a viscous substance. In the first case, we can talk about it as an acute course of a pathological process in the lungs, in the second - about a chronic form of the disease.
- The cough may be dry and make breathing difficult. In some cases, it precedes the occurrence of a wet cough or, conversely, is its consequence. A dry cough itself is a sign of chronic receptor irritation, but fluid does not accumulate in the lungs. It can act as a sign of a progressive tumor, at a stage when inflammation and tissue necrosis are not yet observed around the localized lesion. Treatment is prescribed according to the results of a microbiological study.
- If coughing and hemoptysis suddenly stop, you should urgently consult your doctor, as this is a very dangerous situation. Suppression of the cough reflex indicates the development of intoxication of the body with tumor decay products.
Self-diagnosis and treatment at home can only worsen the situation. It is best to most expressively describe the sensations associated with the disease to your oncologist. The final result is drawn up after a whole range of necessary analyzes and studies have been carried out.
Methods for diagnosing bronchial cancer
Usually the tumor is detected using x-rays. CT and MRI help to clarify its size, location, number of foci and their degree of invasion into surrounding tissues. Bronchoscopy is used - an endoscopic examination, during which a special instrument in the form of a long flexible hose - a bronchoscope - is inserted into the bronchial tree and the mucous membrane is examined.
During bronchoscopy, a biopsy can be performed: a fragment of a pathologically changed area of the mucous membrane can be obtained and sent to the laboratory for cytological and histological examination.
A biopsy can be performed in other ways: using a needle inserted into the lung through the chest wall, during thoracoscopy, or thoracentesis. You can also do a cytological examination of the sputum to look for cancer cells.
PET scanning helps detect small metastases. During this study, sugar with a special radioactive label is introduced into the body. The radiopharmaceutical accumulates in tumor cells and makes the lesions visible in pictures taken using a special device.
If necessary, the doctor may prescribe other diagnostic methods.
Basic diagnostic methods
One of the most common diagnostic methods is radiographic examination. With lung cancer, the image shows a darkened area with unclear edges and processes, and enlarged lymph nodes. To make a correct diagnosis, additional diagnostic methods are often required: computed tomography, bronchoscopy, thoracotomy, biopsy.
Computed tomography allows you to take a more detailed and clear picture of the lungs, which can reveal the presence or absence of cancer.
Bronchoscopy is performed by inserting a tube equipped with a video camera into the airway. This method allows you to detect a tumor and take a piece of material for a biopsy. The test determines whether the sample is in the area of the bronchoscope and performs a needle biopsy. A needle is inserted through the skin to take a sample. Laboratory research methods include sputum testing, tumor marker tests, and general and biochemical blood tests. A cancer patient has an increased ESR and a low hemoglobin level. After taking samples for cancer markers, it is possible to identify not only cancer cells, but also determine the type of pathology. Sputum is checked for the presence of pathogenic microflora.
Surgical treatment of bronchopulmonary cancer
Surgical tumor removal is often the main treatment for local bronchial and lung cancer when there are no isolated metastases. The goal of radical surgery is to completely remove the tumor tissue. Depending on the size and location of the lesions, different types of surgical interventions are used:
- Removal of the entire lung - pneumonectomy .
- Removal of a lobe of the lung - lobectomy .
- Removal of a segment of the lung - segmental resection .
- Removal of the tumor with some surrounding healthy tissue - wedge resection .
- Removal of affected lymph nodes - dissection, lymphadenectomy .
The operation can be performed openly (through an incision) or endoscopically ( video-assisted thoracoscopic surgery , or VATS ).
Radiation therapy
Radiation therapy for bronchial and lung cancer can be combined with surgery. Before surgery, the doctor may prescribe neoadjuvant radiation therapy (including in combination with chemotherapy), this helps to shrink the tumor and make it operable. After surgery, adjuvant chemotherapy is used to kill any remaining cancer cells and reduce the risk of recurrence.
If the tumor is inoperable, radiation therapy becomes the main treatment. For metastatic cancer, it helps fight pain and other symptoms.
Chemotherapy
Chemotherapy drugs are drugs that destroy actively reproducing cells. Thus, their target in the body is primarily tumor cells, but healthy cells can also be affected, which is why chemotherapy is often accompanied by side effects. Modern doctors know how to reduce their risk and how to deal with them.
Like radiation therapy, chemotherapy for bronchial and lung cancer can be adjuvant, neoadjuvant, or can act as the main method of treatment. Different chemotherapy drugs with different mechanisms of action are used. Typically, your doctor will prescribe a combination of two or more drugs. Combinations are selected depending on the type and stage of the tumor.
Lung cancer treatment
Lung cancer therapy is carried out in several ways:
- surgical removal;
- radiation therapy;
- chemotherapy course;
- palliative treatment.
Surgical removal of the tumor
Surgical intervention is performed in the initial stages of the disease, when there is no metastasis. The tumor, fatty tissue, and lymph nodes must be removed; partial excision of nearby organs into which the tumor has grown is required. This method of treatment is contraindicated when distant metastases are present and there is a risk of bleeding.
If surgery cannot be done, patients are prescribed chemotherapy. Drug treatment is also necessary after surgery and radiation therapy. The treatment method is selected individually for each patient, taking into account the form and stage of the disease.
Chemotherapy
Patients are administered intravenously drugs that suppress the growth of cancer cells and immunomodulators. The disease cannot be cured with chemotherapy, but this method can significantly alleviate the patient’s condition and prolong life. Treatment courses are carried out every 3–4 weeks. A total of up to 7 sessions may be required.
Unfortunately, the drugs used for chemotherapy have a detrimental effect not only on cancer cells, but also on the entire human body, so such treatment has many side effects. After courses of chemotherapy, there may be disruption of the digestive tract (nausea, vomiting, diarrhea), the mucous membranes of the oral cavity are affected (stomatitis), hair loss, neuropathies develop, and secondary infections occur.
The effectiveness of chemotherapy depends on the stage at which treatment was started, the general condition of the body, and the qualifications of the attending physician.
Palliative treatment
When surgery and chemotherapy are contraindicated, patients are prescribed supportive treatment aimed at alleviating the symptoms of the pathology. Shortness of breath, cough, hemoptysis, and pain are reduced. The effects of chemotherapy are removed. Patients are provided with care at home under the supervision of a local doctor, in a hospital or hospice.
Lung cancer is a dangerous and serious disease that is difficult to treat. More than 80% of patients die within 2 years after its diagnosis. If the pathology was detected early, after surgical treatment and chemotherapy there is a possibility of extending the patient’s life by 5–15 years.
Targeted therapy and immunotherapy
Targeted therapy and immunotherapy are modern, youngest trends in cancer treatment, the emergence of which became possible thanks to the rapid development of molecular genetics in recent decades:
- Targeted drugs affect a specific target molecule that cancer cells use for survival, uncontrolled reproduction, and activation of blood vessel growth. They act more targeted and selective compared to classical chemotherapy drugs, and due to this they are safer, but still have some side effects.
- The most commonly used immunotherapy drugs checkpoint —molecules that cancer cells use to suppress the immune system.
Typically these treatments are used in later stages when there are metastases. Also, in the later stages, doctors have to deal with such a complication of bronchial and lung cancer as pleurisy.
Differential diagnosis of lung cancer and pneumonia
The difficulty of identifying obstructive pneumonitis and its differentiation from chronic pneumonia is indicated by the following figures: in 1969, according to F.G. Uglova and T.T. Bogdan, 91% of patients with cancer pneumonia were initially diagnosed with chronic pneumonia. Out of a thousand, in 452 patients the error was not detected for more than a year.
Today, half of those who die from undiagnosed lung cancer have chronic pneumonia listed in their medical records.
Fatal errors are explained by the similarity of symptoms and the fact that lung or bronchial cancer is accompanied by pneumonia.
Clinical symptoms of cancer appear late: at the stage of impaired bronchial drainage function, developed inflammatory process, collapse of the lung walls (atelectasis).
Until this point, regular antibiotics provide temporary improvement. On a radiograph after a course of therapy, 15-20% of patients demonstrate restoration of the patency of the affected bronchus and a decrease in the inflamed area around it.
When determining the disease, radiation diagnostic methods are primarily used:
- large-frame fluorography;
- radiography in two standard projections;
- targeted radiography.
After this, the nature of the darkening is studied. On radiographs, the shadows of the tumor have clear edges, in later stages - with processes. The tumor node does not shrink after a course of antibiotic treatment. Cases of central lung cancer, bronchial cancer with inflammation and pneumonia on a radiograph can be very similar: the opacities in both cases can be homogeneous or heterogeneous. The differences lie in the clear contours of the tumor, sometimes of a bizarre shape, and the pronounced shadow of the hilar node.
If the doctor has doubts, it is recommended to continue the examination using effective differential diagnostic tools:
- computed tomography;
- bronchoscopy;
- bronchography.
One of the above-mentioned hardware diagnostic methods is assigned to standard X-ray projections. The choice depends on the age and condition of the patient. Patients over 65 years of age usually do not undergo bronchography.
There are a number of contraindications for bronchoscopy, including: hypertension, exacerbation of asthma, strokes and heart attacks, mental illness. High-resolution tomograms and bronchograms most clearly demonstrate the difference between opacities in pneumonia and cancer.
At the stage of clarifying the diagnosis, a course of intensive anti-inflammatory drug therapy is started. If there is no significant improvement in the first 2 weeks, there are prerequisites for an oncological diagnosis.
Disease markers are looked for in samples:
- sputum;
- washouts of the bronchial mucosa;
- tissue biopsies.
Based on the results of the examination, pneumonia is determined by:
- acute onset;
- physical inflammatory phenomena;
- rapid therapeutic effect from taking antibiotics;
- positive change on the x-ray 14 days after the start of the course.
Signs that help diagnose focal lung lesions were tabulated by Professor of the Belarusian State Medical University, Head of the 1st Department of Internal Diseases A.E. Makarevich.
Table 1. Differential diagnosis of focal lung lesions.
Signs that help diagnose focal lung lesions were tabulated by Professor of the Belarusian State Medical University, Head of the 1st Department of Internal Diseases A.E. Makarevich.
Table 1. Differential diagnosis of focal lung lesions.
| Sign | Focal pneumonia | Peripheral lung cancer |
| Age | At any age, but more often in people under 50 years of age | More common in people over 50 years of age |
| Floor | Equally common in men and women | More common in male smokers |
| Onset of the disease | Usually acute with fever | May be unnoticeable or with increased temperature |
| Cough | At first there may not be | Often absent |
| Dyspnea | With large damage to lung tissue | May be missing |
| Hemoptysis | Rarely | Rarely |
| Chest pain | Occurs when the pleura is involved | Possible |
| Intoxication | Not expressed | Often not expressed |
| Physical data | Pronounced: the breathing pattern changes and moist rales appear | Scanty or absent |
| Laboratory data | Leukocytosis, an increase in ESR, which decreases after the resolution of pneumonia | Moderate increase in ESR with normal leukocyte count |
| X-ray data | Sharply expressed, the lower lobes are more often affected, focal shadows are homogeneous, the boundaries are blurry, increased pulmonary pattern, enlarged roots of the lung | Initially, the shadow of the tumor is low-intensity with unclear contours and “antennae” |
| Effect of antibiotics | Expressed, reverse development of the process after 9-12 days | There is no or false positive dynamics, but changes during X-ray examination persist |