Foreign body of the maxillary sinus
A foreign body of the maxillary sinus is a foreign object located in the maxillary (maxillary) sinus. Its presence can be asymptomatic or with a variety of clinical manifestations - deterioration in general health, pain, fever, nasal congestion, purulent discharge, nosebleeds. The diagnosis is made on the basis of complaints, anamnestic data, physical examination and imaging studies - radiography, CT, direct and endoscopic rhinoscopy. Treatment consists of removing the foreign body surgically, rinsing the sinuses, as well as carrying out antibacterial and anti-inflammatory therapy.
Treatment of foreign body VChP
Most often, parents of young children deal with the problem of a foreign body in the nose.
Children often push various things into their respiratory canals for themselves or their friends. Let's look at their types:
- live - insects;
- inorganic - toys, paper, wood or beads;
- metal - buttons and paper clips, coins or batteries;
- organic - fruit seeds, sunflower seeds, vegetables and so on.
https://www.youtube.com/watch?v=ytpressru
Also, foreign bodies in the nose (ICD-10 code: T17) can be divided into radiopaque and low-contrast. The latter are difficult to see in the picture; these include plastic and wood. Sometimes foreign objects can be passed through the choana during vomiting. Often, after various medical interventions, cotton wool and gauze may remain in the nose.
In adults, foreign bodies get stuck in the sinuses, which is much more serious. Causes include injury or dental procedures.
The main treatment is surgical removal of the foreign object from the paranasal sinus. Depending on the size of the facility, the equipment of the clinic and the qualifications of the doctor, different surgical techniques are used. After removing the foreign body, the sinus cavity is washed. If a bacterial infection is present, antibacterial drugs are prescribed. Penicillin antibiotics are effective - amoxicillin, amoxicillin/clavulanic acid. To reduce swelling of the mucous membrane, vasoconstrictors (decongenants) are used - oxymetazoline, xylometazoline. Methods for surgical removal of a foreign body are divided into two groups:
- Radical. Caldwell-Luc maxillary sinusotomy is performed under local or general anesthesia. During this operation, an incision is made in the gum above the maxillary sinus, trephination of the inert wall, biting and removal of the bone plate. Then the foreign body is removed and the mucous membrane is scraped out. An artificial opening (ostium) is created between the sinus and the nasal cavity. However, this method has a high frequency of complications in the form of impaired sensitivity of the upper lip and recurrence of sinusitis.
- Minimally invasive. These are more gentle methods using endoscopic instruments. Performed under local anesthesia. With microsinusrotomy, the incision and burr hole are small (about 8 millimeters). With trocar maxillary sinusotomy, not an incision is performed, but a one-step puncture of the mucous membrane and bone, due to which the edges of the wound are completely closed, which prevents blood from entering the sinus from the wound. The small size of the surgical wound ensures faster healing and a lower incidence of complications. The least invasive and traumatic is endonasal maxillary sinusotomy, in which no puncture or trepanation of the sinus wall is performed, but instruments are inserted through the natural connection of the sinus and nasal cavity.
Removal of laryngeal foreign bodies
Foreign bodies in the larynx must be removed as a matter of urgency. If asphyxia develops, tracheostomy is required to restore breathing. Subsequently, the patient is transported to the hospital, where the foreign body is removed using intubation anesthesia through a tracheostomy.
It is also advisable to remove non-obstructive foreign bodies of the larynx immediately, since swelling and inflammation of the larynx that develop over time make it much more difficult to remove foreign objects from it. Removal of foreign bodies of the larynx is carried out using laryngoscopy and only in stationary conditions. In adults, the removal procedure is carried out under local anesthesia; in children, it is carried out after the administration of phenobarbital, since the local administration of an anesthetic can reflexively cause them to stop breathing.
The most difficult task is the removal of foreign bodies of the larynx that have penetrated into the pyriform sinuses, ventricles and subglottic space. If it is impossible to remove them naturally, surgical treatment is indicated. The intervention is most often performed by tracheostomy. During this operation, a tracheostomy may be used to remove a foreign body from the larynx or push it upward. If wider access to the structures of the larynx is necessary to remove a foreign body and eliminate its complications (for example, to open an abscess), a laryngotomy is performed. Surgical removal of laryngeal foreign bodies can be complicated by cicatricial stenosis.
Removal of laryngeal foreign bodies is carried out against the background of sedative, anti-inflammatory and analgesic therapy. To prevent infectious complications, systemic antibiotic therapy is necessary.
Treatment of foreign bodies of the larynx, even small ones, pose a danger to life, since a feature of the tissues of the larynx and its reflexogenic zones is the rapid occurrence of obstructive edema and almost instantaneous reflex laryngospasm. Therefore, in all cases of non-obstructive foreign bodies of the larynx, an ambulance should be immediately called or the victim should be transported by improvised transport to the nearest medical institution that has an endoscopist or an ENT specialist. Removal of foreign bodies is carried out only under visual control at the earliest possible time in order to prevent the occurrence of edema, which sharply complicates the extraction procedure and is fraught in some cases with traumatic complications (rupture of the mucous membrane, vestibular or vocal fold, subluxation of the cricoarytenoid cartilage, etc.). Only in the event of asphyxia when foreign bodies are localized in the laryngopharynx before the arrival of a health worker is it permissible to attempt to remove it with a finger, in which, however, it is possible to push the foreign bodies into the deeper parts of the larynx. Some authors recommend striking the back of the neck with the edge of the palm to dislocate foreign bodies and expel them. Probably, the mechanism of such removal is the transfer of shock wave energy to the internal tissues of the neck in the direction of foreign bodies and its propulsion into the oropharynx. Asphyxia can be prevented by tracheotomy or intercricothyroidal laryngotomy, which restores life-saving breathing “at the tip of a scalpel.” Removal of wedged foreign bodies is carried out after tracheotomy, while the tracheostomy is used for intubation anesthesia. The position of the victim and the procedure for direct laryngoscopy are described above. In young children, direct laryngoscopy and removal of foreign bodies are performed without local anesthesia, which is fraught with reflex respiratory arrest, and under premedication with phenobarbital, which acts as an anticonvulsant, and chloral hydrate. The most difficult to remove are foreign bodies wedged into the ventricles of the larynx, pyriform sinuses and subglottic space. Removal of such foreign bodies is carried out after a tracheotomy, and the tracheotomy opening can serve to push the foreign bodies upward or remove them through the tracheostomy. When foreign bodies in the larynx are removed, a reflex cessation of breathing may occur, for which the medical staff must be prepared, having at their disposal the necessary means to restore respiratory function (oxygen, carbogen, respiratory analeptics - lobeline, cititon, etc.). For chronic foreign bodies of the larynx, thyrogomy with preliminary tracheotomy is indicated, especially in the presence of granulations, bedsores and ulcers or phenomena of chondroperichondritis, perforation of the larynx. This surgical intervention has two goals - removal of foreign bodies and sanitizing manipulations to eliminate secondary complications. In all cases of foreign bodies in the larynx, the prescription of broad-spectrum antibiotics is indicated to prevent secondary complications, as well as sedatives, analgesics and, in some cases, tranquilizers.
Foreign bodies of the pharynx
, as a rule, come from food (fish bones, cereal husks, pieces of wood, etc.), less often fragments of dentures, pins, nails get stuck (from tailors, shoemakers). If there is insufficient chewing and hasty swallowing, large pieces of food can get stuck above the esophagus, block the entrance to the larynx and cause asphyxia. Conversation and laughter while eating contribute to the entry of foreign bodies. Most often, sharp foreign bodies get stuck in the area of the pharynx, tonsils and root of the tongue, less often in other parts of the pharynx.
Code according to the international classification of diseases ICD-10:
- T17. 2 - Foreign body in the pharynx
Symptoms, course
Feeling of something foreign in the throat, pain and difficulty swallowing. With large foreign bodies, speech and breathing are impaired. With a long stay of a foreign body, an inflammatory process develops, sometimes with the formation of phlegmon.
Symptoms
The following symptoms are typical for patients who have aspirated foreign bodies. A healthy child suddenly develops a sharp paroxysmal cough, asphyxia, sometimes with loss of consciousness and cyanosis of the facial skin. Characterized by stenotic breathing with retraction of the yielding areas of the chest, frequently recurring bouts of coughing, and hoarseness of the voice. The intensity of the cough depends on the shape, size, nature and location of the foreign body. When a foreign body is fixed, the cough is usually less intense. With foreign bodies of the tracheobronchial tree, stenosis can be fulminant, acute, subacute and chronic. Fulminant stenosis occurs when a foreign body is wedged into the glottis. Acute stenosis is caused by a foreign body in the larynx or trachea. Acute tracheal stenosis is most often caused by a large foreign body localized in the area of tracheal bifurcation and closing the lumen of the bronchi. Subacute stenosis is observed when the bronchus is partially blocked, for example by beans, chronic - when a foreign body is wedged into the bronchus with partial blockage of its lumen. The condition of children with a foreign body in the larynx is often severe. When aspirating a small sharp foreign body (sewing needle, fish bone), at the first moment it enters the larynx, sometimes no breathing disturbance is observed; the phenomena of stenosis in such cases occur much later as a result of the development of reactive edema of the laryngeal mucosa, leading to asphyxia. When aspirating foreign bodies of a pointed or angular shape, which with a sharp end can wedge into the thickness of the mucous membrane of the larynx and disrupt its integrity, pain in the throat and behind the sternum is possible, aggravated by coughing and sudden movements. An admixture of blood appears in the sputum. Important symptoms indicating a foreign body in the larynx are shortness of breath and voice dysfunction. The latter can be short-term or long-term. Persistent hoarseness, as well as aphonia, indicate the localization of a foreign body in the glottis or subglottic space; a rough voice and slight hoarseness indicate injury to the vocal folds during the passage of a foreign body. The most common symptom of a foreign body in the larynx is pronounced attacks of whooping cough, which sometimes lasts a long time, with pauses of varying lengths. Older children may experience foreign body sensation and pain when swallowing. On auscultation, harsh breathing and rough wire-like rales are heard in both lungs, more so in the upper sections. Chest X-ray usually reveals increased transparency of the lung tissue without focal and infiltrative changes. Foreign bodies of the trachea are common; they (for example, watermelon seeds) easily move in the tracheobronchial tree and cause paroxysmal whooping cough. Breathing disturbances are not as pronounced as when foreign bodies are localized in the larynx, and periodically intensify due to the balloting (movement) of the foreign body at the moment of its contact with the lower surface of the true vocal folds. The cough may be intermittent and worsen at night and when the child is restless. Sometimes coughing attacks are expressed sharply, accompanied by cyanosis of the face and vomiting, reminiscent of whooping cough, which often causes diagnostic errors, especially when the moment of aspiration of a foreign body is “overlooked.” Balloting of a foreign body is a characteristic sign of unfixed foreign bodies located in the trachea, and is objectively manifested by the symptom of flapping. When the child is restless, crying, laughing or coughing, a flapping sound is clearly heard - the result of a foreign body launching and hitting the walls of the trachea, larynx and vocal folds during movement during inhalation and exhalation. Coughing up a foreign body is hampered by the valve mechanism of the tracheobronchial tree, which consists in expanding the trachea during inhalation and narrowing it during exhalation, as well as the fact that when coughing, a foreign body is thrown to the glottis and, in contact with the lower surface of the vocal folds, causes closure of the glottis and spasm of the larynx . The following deep breath again carries the foreign body into the lower parts of the trachea. The mucous membrane in the area of the tracheal bifurcation is characterized by increased sensitivity to external irritations compared to the mucous membrane throughout the rest of the respiratory tract. Therefore, when a foreign body is localized in the bifurcation area, the cough is especially pronounced and lasts a long time. When a foreign body significantly blocks the lumen of the trachea or bronchus and the exhaled air passes through the gap formed between the surface of the object and the wall of the trachea or bronchus, a whistle similar to that in bronchial asthma can be heard. With foreign bodies in the bronchi, a distinction is made between through, valve and complete blockage. In cases of through blockage, the foreign body does not completely close the lumen of the bronchus. Breathing is not impaired. The inflammatory process in the lung tissue is moderate. Valve blockage is characterized by the fact that the foreign body is in loose contact with the walls of the bronchus and, when inhaling, air penetrates into the lung. When you exhale, it does not come out due to contraction of the bronchial muscles. Thus, air is trapped in the lung, causing emphysema. Due to complete blockage of the bronchus by a foreign body, obstructive atelectasis develops in the lung. When a foreign body passes through the bronchus, breathing becomes free, coughing occurs less frequently and has a shorter duration, and the child calms down. The localization of a foreign body in the bronchus depends on its size. Large foreign bodies are retained in the main bronchi, small ones penetrate into the lobar and segmental bronchi. In this case, it is usually not possible to establish any characteristic subjective signs. On the side of the obstructed bronchus, more forced breathing is heard, as if overcoming an obstacle; in the area of localization of the foreign body, shortening of the percussion sound, weakening of breathing and vocal tremors are noted. But sometimes dry and even wet rales are heard. If a foreign body remains in the bronchus for a long time, sputum production is observed; its quantity and quality depend on secondary changes in the lung and tracheobronchial tree. X-ray examination reveals signs of impaired bronchial conduction - a symptom of displacement of the mediastinal organs towards the obstructed bronchus, atelectasis of a segment or lobe of the lung in accordance with the level of localization of the foreign body, emphysematous changes in the lungs with ventricular bronchial stenosis. With atelectasis, as with emphysema, symptoms of respiratory failure may occur. If there is complete obstruction of one of the main bronchi, then the corresponding lung is switched off from the act of breathing. As a rule, atelectasis of the corresponding lung is accompanied by cardiovascular failure. Atelectasis of a segment of one lung can occur along with emphysema in the other lung with a displacement of the mediastinal organs to the painful side. Emphysema is accompanied by shortness of breath and pathological disorders of the cardiovascular system. Later, along with atelectasis, bronchitis or pneumonia develops. However, with complete or valvular closure of the bronchi and disruption of their drainage function, chronic pneumonia can develop, in which an inflammatory process is determined at the site of fixation of the foreign body.
Symptoms of foreign bodies in the larynx
Clinical manifestations of laryngeal foreign bodies may vary depending on their consistency, shape and size. Small foreign bodies when they enter the larynx cause a convulsive cough, cyanosis of the skin of the face and difficulty breathing. If a foreign body enters the larynx, reflex vomiting may occur. However, coughing up or vomiting a foreign object is observed only in rare cases. If a foreign body remains in the larynx, hoarseness of the voice develops and pain appears in the larynx. In some cases, pain occurs only when talking or coughing, in others it is constant and intensifies during conversation. Over time, coughing attacks recur again. Foreign bodies of the larynx located between the vocal folds prevent their closure and lead to aphonia.
Small foreign bodies of the larynx are initially not accompanied by respiratory problems and for a long time can manifest themselves only as hoarseness and periodic coughing. Over time, inflammation begins to develop in the area where they occur, leading to progressive swelling and narrowing of the lumen of the larynx, resulting in breathing difficulties. The addition of a secondary infection is accompanied by a rise in body temperature and the appearance of mucopurulent sputum.
Foreign bodies of the larynx of significant size and elastic consistency (removed adenoids, cotton swabs, poorly chewed pieces of meat) immediately obstruct the lumen of the larynx, leaving no space for air to pass through. In this case, in a matter of seconds, the victim’s face acquires a cyanotic hue, and extreme fear is expressed on it. The person begins to rush about, wheezes and makes convulsive breathing movements, which, due to obstruction, do not lead to air entering the respiratory tract. After 2-3 minutes, a coma occurs. If it was not possible to eject the foreign body or restore breathing through tracheostomy, then after 7-9 minutes respiratory and cardiac arrest may occur, leading to death. When respiratory and cardiac activity is restored a few minutes after the development of asphyxia, there is a danger that, as a result of prolonged oxygen starvation, the cortical centers of the brain are switched off.
Diagnostics
A foreign body in the respiratory tract is recognized not only on the basis of a carefully collected history, objective data, and knowledge of the main clinical manifestations of aspiration of foreign bodies, but also with the help of X-ray examination (tomography, bronchography). For final diagnosis, endoscopic methods (bronchoscopy, direct laryngoscopy) are also used. To detect a foreign body in the bronchus, aspiration of purulent contents should be performed using an electric suction, and swelling of the bronchial mucosa should be reduced with a 0.1% solution of adrenaline.
Diagnosis of foreign bodies in the larynx
Laryngeal foreign bodies accompanied by obstructive syndrome are diagnosed by characteristic clinical manifestations and the typical sudden onset of symptoms. If respiratory problems do not require emergency assistance, then to confirm the diagnosis, laryngoscopy is performed, during which it is possible not only to identify, but also to remove a foreign body of the larynx. In children, direct laryngoscopy is used, in adults - indirect.
For foreign bodies in the larynx that occur without breathing problems, patients usually turn to an otolaryngologist a few days after a foreign object enters the larynx. During this time, an inflammatory reaction and swelling of the laryngeal mucosa develops, preventing good visualization of the object. Therefore, in such cases, to detect a foreign body, they resort to tuberculosis, laryngeal papillomatosis.
Differential diagnosis
Foreign bodies of the tracheobronchial tree should be differentiated from laryngotracheobronchitis, pneumonia, acute bronchitis, congenital lobar emphysema, foreign body of the esophagus, acute respiratory disease, etc. As a result of a long stay of a foreign body in the respiratory tract, complications arise, more often in young children. This is often due to a narrowing of the airway lumen, as well as a decrease in the resistance of the lung tissue. In addition, organic foreign bodies, such as peas, often cause bronchopneumonia. Such bronchopneumonia takes a long time and is difficult to treat. One of the very rare and severe complications of foreign bodies in the respiratory tract is a lung abscess. Complications include diseases such as abscess pneumonia, tracheobronchitis, pulmonary atelectasis, pneumothorax, bronchiectasis, and bleeding.
Causes
Foreign bodies in the respiratory tract are a fairly common pathology in childhood. They are divided into inorganic (pacifier, sewing needles, safety pins, coins, parts from toys, nails) and organic (peas, beans, beans, pits from peaches, apricots, cherries, watermelon seeds). Foreign bodies can also be roundworms and leeches. Depending on the shape, size and nature of aspirated foreign bodies, they are localized in various parts of the upper respiratory tract. They usually do not linger in the trachea and in up to 80% of cases end up in the right bronchus. Foreign body aspiration is always unexpected and occurs under a wide variety of conditions. Foreign bodies usually enter the body naturally, less often - during surgical interventions (tracheotomy, adenotomy, removal of a foreign body from the nasal cavity, dental procedures), as well as through penetrating wounds of the chest, neck, or trauma to the larynx. In addition to the usual route (through the mouth), foreign bodies can enter the respiratory tract from the esophagus and stomach during vomiting. Foreign bodies enter the respiratory tract during eating; it is promoted by laughter, talking, crying, sudden fear, coughing, falling, as well as the desire of most children to put all objects in their mouths. At the moment of a sharp inhalation, foreign bodies located in the mouth are carried inward by a strong inspiratory stream of air. Foreign bodies in the respiratory tract are more often observed in young children due to the poor development of their protective reflexes - spasm of the entrance to the larynx and spasm of the glottis, followed by a reflex cough. In young children, the larynx is located very high, the distance from the teeth to the entrance to the larynx is small. In addition, there is underdevelopment of reflexogenic zones in the area of the true and false vocal folds, in the subglottic space, and in the area of the epiglottis. The above reasons contribute to the penetration of foreign bodies into the larynx. Pathological changes in the respiratory tract depend on the nature and size of the foreign body, as well as on the time it remains in the respiratory tract. When an acute metal foreign body is introduced, hyperemia, swelling of the mucous membrane, and exudation phenomena are observed locally. Late local signs of a foreign body include the formation of a capsule around it, its sclerosis, the proliferation of granulations with their subsequent scarring.
Complications of foreign bodies in the larynx
Foreign bodies of the larynx often cause an inflammatory process at the site of their localization. The severity of the inflammatory reaction depends on the type of foreign bodies in the larynx, their infection and the duration of their presence in the larynx. The presence of foreign bodies in the larynx for a long time leads to the formation of contact ulcers, bedsores, granulomas and secondary infection. Sharp foreign bodies in the larynx can cause perforation and migrate to adjacent anatomical structures. The resulting perforation can cause mediastinal emphysema, and also contributes to the spread of secondary infection with the development of perilaryngeal or retropharyngeal abscess, perichondritis, mediastinitis, jugular vein thrombosis, sepsis.
Large foreign bodies of the larynx, as well as accompanying swelling of the mucous membrane and reflex spasm of the laryngeal muscles, can cause complete closure of the lumen of the larynx and asphyxia, leading to the death of the patient.
Treatment
Any foreign body must be removed. A child with a foreign body in the respiratory tract should be immediately hospitalized in a hospital. If the child is in a state of acute asphyxia, then for health reasons an immediate tracheotomy is necessary (the operation is performed by a doctor). Parents and the child’s closest relatives, having suspected foreign body aspiration, should seek help from any medical institution, in particular to a paramedic and obstetric station. In all cases, if there is no suffocation, the paramedic, if a foreign body is suspected in the respiratory tract, is obliged to refer the child to the laryngology department. The paramedic must be able to assist the doctor in removing a foreign body from the respiratory tract. A child with a foreign body in the respiratory tract is taken to the hospital by ambulance. During the journey, children with floating foreign bodies in the trachea must be placed in a sitting position to avoid movement of the foreign body and asphyxia. If necessary, artificial respiration is performed, cardiovascular drugs and tsititon are administered, and oxygen is given to breathe. In children, a foreign body in the trachea or bronchi is removed using upper bronchoscopy (under endotracheal anesthesia using muscle relaxants). In case of strongly wedged foreign bodies, it is necessary to perform a tracheotomy or lower bronchoscopy. With a wedged foreign body of the bronchus (lobar or segmental) in young children, bronchial rupture with infection of the mediastinum is possible. Sometimes in such cases they resort to thoracotomy. To prevent swelling of the subglottic space, immediately after upper bronchoscopy, 50-100 mg of hydrocortisone and diprazine in an age-specific dosage are administered intravenously.
First aid
The health and life of a person often depends on how quickly first aid is provided. At the same time, self-medication is possible only if the child understands what people require of him and can freely follow the instructions of adults. If the child is under 3 years old, it is better to take him to the hospital immediately so as not to waste time.
Before removing a foreign body from the nose, you need to understand how far it is stuck. If it is visible to the naked eye, then you need to introduce special drops into the nose that constrict the blood vessels. After 5 minutes, you need to ask the baby to blow his nose. In this case, you should help him by closing the free nostril. If this procedure was ineffective, then you need to provoke sneezing. If both methods do not help, then you need to take the child to the hospital.
If an insect gets into your nose, it is better to consult a doctor immediately. This is because it can creep further and create serious problems. If the object was pulled out, you should also contact a specialist. We will have to do special tests that will make it possible to understand whether the mucous membrane is damaged and whether there are any fragments of the object left in the nose. After this, you need to take an antibacterial course to prevent inflammation.
It should be understood that most often the foreign body is removed on an outpatient basis. Before performing this procedure, local anesthesia is given. Next, vasoconstrictor drops are administered. Then wait 15 minutes for the drops to take effect. Then the nasal passages are examined and objects are pulled out using a hook or forceps.
If the child is very small, then he is given general anesthesia, since it is impossible to make him sit still. Full anesthesia is also sometimes prescribed for children who do not respond to local anesthetics. After the object is removed, the doctor prescribes a special therapy that will relieve inflammation and relieve symptoms.
The treatment regimen will depend entirely on how long the foreign body was in the child’s nose. Most often, antibiotics are prescribed in the form of “Suprax”, “Ampicillin” and others. In order to restore the mucous membrane and relieve swelling, Dolphin or Morenasal are prescribed. Calcium-containing medications are also often used.
Forecast
When correctly removing an object from the nose, the prognosis is generally positive. If the object had sharp parts or corners, then injury to the mucous membranes can lead to various types of complications. If treatment is not carried out, the risk of developing other pathological conditions increases significantly.
How to remove a foreign body in a child’s nose:
Foreign bodies of the larynx
- foreign objects of various natures that accidentally end up in the larynx. Foreign bodies in the larynx can be small household objects, parts of food, living organisms, medical instruments or parts thereof. Foreign bodies of the larynx manifest themselves in varying degrees of severe respiratory disturbances, hoarseness or complete aphonia, paroxysmal cough, and pain in the larynx. Their diagnosis is based on a typical clinical picture, direct and indirect laryngoscopy, microlaryngoscopy, and radiological data. The treatment strategy consists of urgent removal of foreign bodies in the larynx. The removal technique depends on the size and location of foreign objects. This may be laryngoscopy, tracheotomy or laryngotomy.
What is prohibited?
If parents are trying to pull a foreign object out of the nose, it is necessary to understand that this event is the most serious. Any wrong action can lead to a worsening of the condition. That is why it is necessary to take measures to prevent the development of complications.
Do not press on the nostril on the affected side, use tweezers or a cotton swab when removing a foreign object, and do not rinse your nose with any liquid. Trying to crush a foreign body in the nose is also not worth it, especially if a person tries to do this with a sharp and long object. Otherwise, all this could end with very disastrous consequences. Such “help” can lead to serious injuries that will lead to inevitable surgery.
Why is a foreign body in the nose dangerous?
First of all, a foreign body in the nasal sinus is dangerous precisely because of the increased risk of the object moving into the pharynx or larynx, which can lead to suffocation.
But keeping an object in the nasal passage for a long time leads to:
- Ulceration of the mucous membrane;
- Necrosis of the nasal concha;
- Suppuration of the lacrimal sac;
- Impaired functionality of the tear ducts;
- Attachment of a secondary infection;
- Purulent rhinosinusitis;
- Osteomyelitis of the nasal bones;
- Perforation of the nasal wall.
The longer treatment is not carried out, the higher the risk of developing severe pathological conditions.
Which specialist should I contact?
https://www.youtube.com/watch?v=ytcreatorsru
Only an otolaryngologist is involved in removing a foreign object. If such a specialist is not available, then you urgently need to look for a therapist or surgeon. You can also go to a 24-hour emergency room.
If such a problem occurs at night or there is no way to go to the hospital, then you need to call an ambulance, which will send an otolaryngologist to your home. In addition, the operator will advise you in detail and tell you what to do.
Differential diagnosis
Foreign bodies of the tracheobronchial tree should be differentiated from laryngotracheobronchitis, pneumonia, acute bronchitis, congenital lobar emphysema, foreign body of the esophagus, acute respiratory disease, etc. As a result of a long stay of a foreign body in the respiratory tract, complications arise, more often in young children.
This is often due to a narrowing of the airway lumen, as well as a decrease in the resistance of the lung tissue. In addition, organic foreign bodies, such as peas, often cause bronchopneumonia. Such bronchopneumonia takes a long time and is difficult to treat. One of the very rare and severe complications of foreign bodies in the respiratory tract is a lung abscess.
Attention!
- By self-medicating, you can cause irreparable harm to your health.
- The information posted on the MedElement website and in the mobile applications “MedElement”, “Lekar Pro”, “Dariger Pro”, “Diseases: Therapist’s Guide” cannot and should not replace a face-to-face consultation with a doctor. Be sure to contact a medical facility if you have any illnesses or symptoms that concern you.
- The choice of medications and their dosage must be discussed with a specialist. Only a doctor can prescribe the right medicine and its dosage, taking into account the disease and condition of the patient’s body.
- The MedElement website and mobile applications “MedElement”, “Lekar Pro”, “Dariger Pro”, “Diseases: Therapist’s Directory” are exclusively information and reference resources. The information posted on this site should not be used to unauthorizedly change doctor's orders.
- The editors of MedElement are not responsible for any personal injury or property damage resulting from the use of this site.
Foreign bodies of the pharynx
, as a rule, come from food (fish bones, cereal husks, pieces of wood, etc.), less often fragments of dentures, pins, nails get stuck (from tailors, shoemakers). If there is insufficient chewing and hasty swallowing, large pieces of food can get stuck above the esophagus, block the entrance to the larynx and cause asphyxia. Conversation and laughter while eating contribute to the entry of foreign bodies. Most often, sharp foreign bodies get stuck in the area of the pharynx, tonsils and root of the tongue, less often in other parts of the pharynx.
Code according to the international classification of diseases ICD-10:
- T17. 2 - Foreign body in the pharynx
Symptoms, course
Feeling of something foreign in the throat, pain and difficulty swallowing. With large foreign bodies, speech and breathing are impaired. With a long stay of a foreign body, an inflammatory process develops, sometimes with the formation of phlegmon.
Diagnostic methods
Most often, if parents do not go to the doctor immediately, but after some time, diagnosis becomes very difficult. This is due to the fact that the object is securely fixed in the nose and a period of remission begins. In order to detect it, you need to perform a special procedure called rhinoscopy.
It is most difficult to diagnose this problem in those children who cannot or are afraid to talk about what they feel, or if they simply do not feel the presence of a foreign body in the nose. In such cases, an x-ray is prescribed in 3 projections.
If the object is poorly visible, then contrast agents are used together with computed tomography. Thanks to this method, you can identify any object, as well as understand and distinguish it from sinusitis or diphtheria.
In order to protect children, it is necessary to constantly monitor their activities. However, there are cases when it is impossible to provide round-the-clock supervision, especially if the child is not the only one. Therefore, there are preventive measures that will help reduce the likelihood of such a problem occurring.
Children should not be left unattended when they are in a room with small objects. You also need to remember that toys such as construction sets are for children over 3 years old. That is why younger children should not buy them. The same applies to collapsible dolls and cars.
Also, before giving fruit to your child, you need to remove the seeds from them. It is necessary to remove all small items from shelves and surfaces where children can reach them. Unless, of course, you want your child to stuff a bead or paperclip up his nose.
If we are talking about children of preschool and primary school age, then it is necessary to conduct conversations that will keep them safe on the street and at home, and it is necessary to explain what the consequences may be if they do not listen.
In adults, preventive measures come down to constantly taking care of your teeth and avoiding facial injuries.
In most cases, the prognosis is favorable. If you seek medical help in a timely manner, the development of serious complications is extremely rare. Before performing endodontic interventions on the upper jaw, it is advisable to conduct a computed tomography scan to determine the thickness of the alveolar process between the tooth root and the maxillary sinus.
Causes
Foreign bodies in the respiratory tract are a fairly common pathology in childhood. They are divided into inorganic (pacifier, sewing needles, safety pins, coins, parts from toys, nails) and organic (peas, beans, beans, pits from peaches, apricots, cherries, watermelon seeds). Foreign bodies can also be roundworms and leeches.
https://www.youtube.com/watch?v=upload
Depending on the shape, size and nature of aspirated foreign bodies, they are localized in various parts of the upper respiratory tract. They usually do not linger in the trachea and in up to 80% of cases end up in the right bronchus. Foreign body aspiration is always unexpected and occurs under a wide variety of conditions.
Foreign bodies usually enter the body naturally, less often - during surgical interventions (tracheotomy, adenotomy, removal of a foreign body from the nasal cavity, dental procedures), as well as through penetrating wounds of the chest, neck, or trauma to the larynx. In addition to the usual route (through the mouth), foreign bodies can enter the respiratory tract from the esophagus and stomach during vomiting.
Foreign bodies enter the respiratory tract during eating; it is promoted by laughter, talking, crying, sudden fear, coughing, falling, as well as the desire of most children to put all objects in their mouths. At the moment of a sharp inhalation, foreign bodies located in the mouth are carried inward by a strong inspiratory stream of air.
Foreign bodies in the respiratory tract are more often observed in young children due to the poor development of their protective reflexes - spasm of the entrance to the larynx and spasm of the glottis, followed by a reflex cough. In young children, the larynx is located very high, the distance from the teeth to the entrance to the larynx is small.
In addition, there is underdevelopment of reflexogenic zones in the area of the true and false vocal folds, in the subglottic space, and in the area of the epiglottis. The above reasons contribute to the penetration of foreign bodies into the larynx. Pathological changes in the respiratory tract depend on the nature and size of the foreign body, as well as on the time it remains in the respiratory tract.
In young children, foreign objects end up in the maxillary sinus due to banal pranks or curiosity, in adults - due to a domestic or work injury, gunshot wound. Also, foreign bodies can enter the sinus during vomiting through the posterior sections of the nasal passages, but this phenomenon is rather casuistry. The most common reason for finding a foreign object in the sinus is iatrogenic, i.e. consequences of medical interventions. The lion's share (more than 80%) is allocated to dental procedures on the teeth of the upper jaw - implantation, prosthetics, filling, etc.
Various factors contribute to the entry of foreign bodies into the sinus during dental procedures. Internal factors include the close location of the bottom of the maxillary sinus to the roots of the teeth and thinning of bone tissue due to existing chronic diseases (diabetes mellitus, maxillary sinus cysts, osteoporosis, hyperparathyroidism, malignant neoplasms, multiple myeloma). External factors are non-compliance with the technique of working with the root canal and insufficient equipment of dental clinics with the necessary equipment and instruments.
Treatment of foreign body VChP
Any foreign body must be removed. A child with a foreign body in the respiratory tract should be immediately hospitalized in a hospital. If the child is in a state of acute asphyxia, then for health reasons an immediate tracheotomy is necessary (the operation is performed by a doctor). Parents and the child’s closest relatives, having suspected foreign body aspiration, should seek help from any medical institution, in particular to a paramedic and obstetric station.
In all cases, if there is no suffocation, the paramedic, if a foreign body is suspected in the respiratory tract, is obliged to refer the child to the laryngology department. The paramedic must be able to assist the doctor in removing a foreign body from the respiratory tract. A child with a foreign body in the respiratory tract is taken to the hospital by ambulance.
During the journey, children with floating foreign bodies in the trachea must be placed in a sitting position to avoid movement of the foreign body and asphyxia. If necessary, artificial respiration is performed, cardiovascular drugs and tsititon are administered, and oxygen is given to breathe. In children, a foreign body in the trachea or bronchi is removed using upper bronchoscopy (under endotracheal anesthesia using muscle relaxants).
In case of strongly wedged foreign bodies, it is necessary to perform a tracheotomy or lower bronchoscopy. With a wedged foreign body of the bronchus (lobar or segmental) in young children, bronchial rupture with infection of the mediastinum is possible. Sometimes in such cases they resort to thoracotomy. To prevent swelling of the subglottic space, immediately after upper bronchoscopy, 50-100 mg of hydrocortisone and diprazine in an age-specific dosage are administered intravenously.
Resection
One of the best methods for eliminating nasal defects after foreign body entry is turbinate resection. It is performed if a person has a deviated septum.
Sometimes, when exposed to any foreign body, a curvature of the cartilage plate appears, which makes breathing difficult. Most often, this procedure is performed on young patients. This is due to the fact that as a person ages, cardiovascular activity is impaired, so there is a great risk when performing such an operation.
The resection is done without any incisions on the face. At the same time, the shape of the outer part of the nose remains the same, that is, no external cosmetic defects remain. If the deformation is quite severe, then the damaged fragment of cartilage is removed and a bone plate is inserted in its place. The operation can be done under general anesthesia, although most often only local anesthesia is used.
Complications
You should understand what complications await a child and an adult if a foreign object is in the nose for a long time. If it is an insect, then even if it does not climb further along the passage, then sooner or later it will die and begin to decompose. Because of this, not only will an unpleasant odor be released, but an inflammatory process will also occur.
If fragile objects are in the nose, they can break down and move further along the respiratory tract. They will end up in the sinuses and throat.
Another serious complication of such an ailment as a foreign body in the nose (ICD code 10: T17) is sinusitis. It may be associated with meningitis, tonsillitis, osteomyelitis and some other serious diseases. That is why the sooner a foreign object is detected in a child or adult and appropriate measures are taken, the less likely it is that inflammation will begin. If the object could not be removed on your own, you should call an otolaryngologist at home.
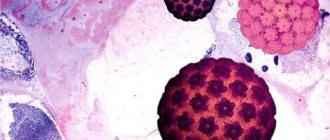
A foreign body in the maxillary sinus, if not diagnosed and treated in a timely manner, can be complicated by a fungal infection (aspergillosis), polyposis and hypertrophic changes in the mucous membrane, sometimes even to the point of complete occlusion of the sinus lumen. Aspergillosis is especially common when ingested by filling material containing zinc oxide and barium sulfate, which inhibit the function of the ciliated epithelium and are a breeding ground for aspergillus fungi.
Pathogenesis
The reaction of the tissues of the maxillary sinus to a foreign object is determined by its characteristics (material, absorbability, presence of sharp edges, sterility or infection) and the immune reactivity of the macroorganism. In rare situations (with very small sizes, smooth edges and low infection), self-removal of a foreign body may occur, first into the nasal cavity through the anastomosis, then from the nasal cavity outward. This is possible due to the functioning of the cilia of the ciliated epithelium of the sinus mucosa. However, in the vast majority of cases, due to constant irritation, an inflammatory process of varying severity develops. The mucous membrane swells and thickens, the lumen of the anastomosis with the nasal cavity overlaps, and the function of the ciliated epithelium is disrupted. When coccal microflora is introduced, massive migration of leukocytes occurs through the vascular wall, and purulent exudate appears. If the object has sharp edges, the mucous membrane is damaged and bleeding develops.