What is nosebleed?
Nosebleeds are a common disease of the ENT organs, which is the leakage of blood from the vessels of the nose as a result of injury, local disease or against the background of a disease of the body. The disease is acute and requires immediate emergency medical care. In case of its absence, this leads to a deterioration in the person’s condition, even to death. Therefore, underestimating this disease and considering it a short-term ailment is a common mistake of patients. There is a well-known fact in history when the leader of the Huns, Attila, did not capture the Roman Empire, dying in Western Europe from a nosebleed.
Technique for stopping nosebleeds in a 10 year old child
1. Sit the victim down, tilt his head forward.
2. Calm down, give a tray to spit out blood.
3.A cold compress is applied to the bridge of the nose.
4.Press the wings of the nose to the nasal septum for 3-5 minutes, without blowing your nose.
5. You can instill Naphthyzin, Glazolin.
6. If bleeding does not stop after 4-5 minutes, insert gauze balls moistened with 3% hydrogen peroxide or 5% aminocaproic acid into the nasal passages.
7. If bleeding continues, it is necessary to perform an anterior nasal tamponade using tweezers or a grooved probe, insert a gauze turunda moistened with 3% hydrogen peroxide or 5% aminocaproic acid into the anterior part of the nose.
8. Apply a sling-shaped bandage to the nose.
9. Admit to the ENT department in a sitting position.
ALGORITHM FOR STOPING BLEEDING after tooth extraction.
1. Sit down and calm the patient.
2.Open his mouth wide.
3. The oral cavity is rinsed with 3% hydrogen peroxide solution, then washed with furacillin solution.
4. A dense lump prepared from cotton wool is used to tamponade the tooth socket. The first and second fingers squeeze the edges of the hole.
5. After this, the patient clenches his jaw tightly and holds it in this state for 20 minutes.
6. After the bleeding has stopped, the tampon is removed from the tooth socket.
ALGORITHM FOR STOPING BLEEDING from the ear canal
insert a turunda made of gauze, moistened with 3% hydrogen peroxide solution or dry, into it, compact it somewhat and apply an aseptic bandage to the ear.
III. Conclusion.
Timely diagnosis of bleeding, immediate adoption of emergency measures to stop it and implementation of emergency measures to eliminate blood loss make it possible to successfully combat this formidable pathological process. The fate of a person depends on how competent the paramedic’s actions are.
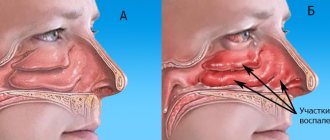
Symptoms and classification of nosebleeds
Signs of a nosebleed are blood draining from the nostrils to the outside or down the back of the throat through the nasopharynx. Bleeding is divided into posterior and anterior. Anterior bleeding affects the Kisselbach capillary plexus, and posterior bleeding comes from large vessels and poses a great danger to the patient.
The main danger to human life is the amount of blood lost. Normally, a healthy person has approximately 4-5 liters of blood in the body. With short-term bleeding, the volume of blood loss is up to 100 ml. This amount of blood loss does not lead to changes in the body, but depending on the type of nervous system, it can manifest as emotional excitement or fainting against the background of vegetative-vascular dystonia.
But if the volume of blood loss is more than 400-500 ml, then the patient develops weakness, dizziness, tinnitus, stars flashing before the eyes, the person becomes pale, the pulse quickens, and the blood pressure rises compensatory. If the blood continues to flow and the volume of lost blood is up to 2-3 liters, then the patient shows signs of hemorrhagic shock. Contact with the patient becomes difficult, shortness of breath increases, the skin turns pale, the extremities become cold, the hands, feet, and lips turn blue. Blood pressure decreases, the pulse is practically not palpable. The patient may lose consciousness.
Nosebleeds of general origin
These bleedings can be dangerous depending on the common causes, of which the most common is hypertension (50%). Bleeding of hypertensive origin is profuse in nature and can often lead to significant blood loss and hypoxic collapse if intervention is not timely.
Other causes include mitral valve stenosis, pulmonary emphysema, liver cirrhosis, kidney and blood diseases, occupational intoxication, vitamin deficiency C, Osler's disease, agranulocytosis, etc. General bleeding is difficult to stop and often recurs, causing anemia.
Causes
This pathological condition is caused by various reasons, but there are two groups of factors leading to nosebleeds.
- Local injuries that are the most common cause of nosebleeds:
- Injury to the nose during sports or an accident;
- Surgery, such as rhinoplasty;
- Interference by foreign objects, including a finger;
- Diseases: allergic and atrophic rhinitis, sinusitis, sinusitis. With such pathologies, the blood vessels of the nose become unprotected and are more often damaged, especially if the mucous membrane is regularly dried out by nasal medications;
- Anatomical deformation of the nasal cavity;
- Ulcerations in the area of Kisselbach's choroid plexus;
- Using drugs by snorting them through the nose;
- Tumors in the nasal cavity or paranasal sinuses: nasopharyngeal carcinoma, bleeding polyp;
- Low air humidity (especially in winter), leading to drying of the nasal mucosa;
- Barotrauma;
- Using an oxygen catheter.
- Systemic causes, which are less common, but require close attention from a doctor:
- Allergy;
- Various infectious diseases: acute respiratory infections, acute respiratory viral infections, influenza, diphtheria, sepsis, accompanied by intoxication of the body. Toxins, viruses and bacteria lead to dilation of blood vessels, which become thin and fragile. Against the background of infections, there is a weakening of blood clotting processes and an increase in the permeability of its elements;
- Arterial hypertension (high blood pressure);
- Vascular diseases, including atherosclerosis;
- Heart failure;
- Increased intracranial pressure;
- Blood diseases: leukemia, capillary toxicosis, hemoblastosis, anemia, hemophilia, hemorrhagic vasculitis, Randu-Osler, Werlhoff, von Willebrand diseases;
- Lack of vitamins K and C in the body;
- Pathological conditions of the liver: hepatitis and cirrhosis, which lead to a decrease in the synthesis of components that affect the normal functioning of the hemostatic system. At the same time, the structure of the liver tissue changes, which causes a slowdown in blood flow and an increase in blood pressure in those vessels that are responsible for renal circulation;
- Abuse of alcoholic beverages that cause vasodilation;
- Angiofibroma, which is a formation localized in the nasopharynx or at the base of the skull. It is characterized by frequent nosebleeds;
- Kidney diseases that cause high blood pressure;
- Hypothyroidism, expressed in dysfunction of the thyroid gland, in which platelet production decreases;
- Side effects of medications.
The main causes of nosebleeds are:
- blood diseases (leukemia, hemophilia, etc.)
- heart disease
- vascular diseases
- kidney disease
- liver disease
- nasal injuries (including nose picking, severe nose blowing)
- tumors
- excitement
- overheating.
Very often, such bleeding is the result of the anatomical structure and location of the vessels supplying the anterior parts of the nose and septum. This is where the Kisselbach-Little zone is located, where the superficial vascular bundle lies. A careless touch is enough to cause bleeding in this area. This often occurs with increased blood pressure.
Malignant or benign tumors located in the nasal cavity often cause nosebleeds. Benign formations include septal polyps, papillomas, angiomas and other formations.
The most common cause of nosebleeds is fragility of blood vessels. Some people note the appearance of blood from the nose even with normal sneezing, and more often this reason is revealed during examination of children under 10 years of age - the body is still growing, so over the years the described syndrome disappears. People with persistent high blood pressure also complain of spontaneous nosebleeds; this syndrome almost always appears with a nasal injury. In general, medicine distinguishes two large groups of causes of nosebleeds - local and systemic.
Local causes of nosebleeds
These include:
Please note: it is not at all necessary that the above factors necessarily lead to the opening of nosebleeds, but they can provoke it. For example, some types of nasal trauma are characterized by the absence of blood discharge, but the presence of swelling, difficulty breathing and other signs of developing pathology.
Systemic causes of nosebleeds
In this case, the appearance of nosebleeds will be influenced by the general state of health and certain chronic pathological processes. Systemic factors that can provoke nosebleeds include:
- diagnosed allergy to any external or internal irritant;
- hypertension is not a periodic increase in blood pressure, but stable hypertension;
- drinking alcohol in large quantities and often - drinks containing alcohol dilate blood vessels;
- chronic diseases of the liver and heart of an inflammatory or infectious nature;
- long-term use of certain medications - in this case, nosebleeds will be classified as a side effect;
- excessive physical exertion, sunstroke, overheating - nosebleeds in this case begin suddenly and are short-lived;
- hormonal disorders - this factor applies more to women; it is not surprising that complaints about the described syndrome come from pregnant women;
- infectious diseases - with measles, scarlet fever, influenza, the permeability of the walls of blood vessels increases.
In addition, nosebleeds can be associated with changes in barometric pressure - a similar syndrome is characteristic of divers, pilots, and climbers.
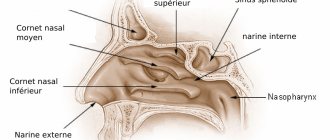
To understand the causes of nosebleeds, it is important to know the anatomical structure of the nose and its functions. The nose and nasal cavity are the upper parts of the respiratory system. When we inhale, the air in the nasal cavity is purified, warmed and moistened. The vasomotor function is performed by an extensive vascular network located in the nasal cavity. When cold and dry air enters the nose, the vessels dilate and become congested, due to which the nasal mucosa thickens and allows less air to pass through in order to warm and moisten it. The opposite processes occur when warm, humidified air enters.
The vessels in the nasal cavity originate from the system of the external and internal carotid arteries. They are responsible for the blood supply to the anterior sections of the nasal septum. The weak point of the nasal vascular system is the anastomosis - the place where capillaries from the external and internal carotid artery systems are connected. There are two such places in the nasal cavity, and both of them are located in the area of the nasal septum. In the anterior sections it is the vascular bundle of Kisselbahi (Locus Kisselbahi), in the posterior sections it is the Woodruff bundle (plexus Woodruff). The vessels in the anastomotic area have a thin wall, covered on top with a thin mucous membrane of the nasal cavity. Therefore, minor injuries, increased pressure, and dry cold air cause damage to these vessels.
The most common cause of nosebleeds is injury. So-called post-traumatic nosebleeds. But in addition to traumatic bleeding, there are iatrogenic causes. They represent nosebleeds after operations, manipulations in the nasal cavity (puncture, catheterization), installation of nasogastric or nasotracheal tubes during anesthesia or gastric lavage, endoscopic examination of the nasal cavity.
A deviated nasal septum, adenoid vegetations, aneurysms of the vessels of the nasal cavity, an oncological process or neoplasms in the nose are all predisposing factors for nosebleeds.
Diseases of internal organs and diseases of the cardiovascular system can also cause nosebleeds. Most often it occurs in patients with hypertension with increased blood pressure. In case of incorrectly selected therapy and the patient does not comply with the doctor’s recommendations to stabilize the pressure, surges occur that lead to damage to blood vessels.
Patients who take anticoagulants (drugs that reduce blood clotting) also often experience nosebleeds.
Ruptures of mucosal capillaries can also occur when:
- colds
- use of narcotic drugs
- frequent use of vasoconstrictor drugs
- being in dry and cold climates
- overheating of the body (sunstroke)
- for vitamin deficiencies (vitamin C deficiency)
- when drinking alcohol in large quantities
- rapid immersion in water or climbing a mountain
In some cases, nosebleeds result from trauma to the nose.
Nosebleeds may be associated with:
- with damage to the integrity of the vessel wall due to injury or increased permeability;
- with pathology in the blood coagulation system.
Methods to stop nosebleeds
Previous7Next
In case of moderate nosebleeds, when we see the bleeding vessel, the bleeding can be stopped using the following methods and methods.
Apply chemical agents to a bleeding vessel:
• vasoconstrictor drugs (0.1% solution of adrenaline hydrochloride or solutions of glazolin 0.1%, naphthyzine 0.1%, norepinephrine hydrotartrate 0.2%, mezatone 1%, ephedrine hydrochloride 2-5%, etc.);
• 3% hydrogen peroxide solution;
• 5% solution of e-aminocaproic acid;
• trichloroacetic acid;
• 10, 20, 30%, or 50% silver nitrate solution;
• 7% collargol solution;
• 36% aqueous solution of polymethylene methacresol sulfonic acid (“Vagotil”).
Influence the bleeding vessel with physical factors:
• press the wing of the nose to the nasal septum;
• apply an ice pack to the nose area;
• perform cryotherapy or perform diathermocoagulation;
• perform ultrasonic disintegration (previously, the affected area is infiltrated with a solution of novocaine, which creates optimal conditions for the introduction of an ultrasonic probe);
• under endoscopic control, perform bipolar coagulation of the bleeding vessel.
In case of significant nosebleeds, as well as their recurrence, the main way to stop is tamponade (anterior or posterior) of the nasal cavity, which can only be fully carried out by an otolaryngologist. Only after it are carried out certain general therapeutic measures. Before tamponade of the nasal cavity, anesthesia of the mucous membrane should be performed.
Anterior tamponade. The nasal cavity is filled with a long gauze swab 1-1.5 cm wide soaked in petroleum jelly, which is inserted with a nasal forceps, curved tweezers or a thin hemostatic clamp using a nasal speculum under visual control (Fig. 18-1 a). A method to prevent tampons from entering the nasopharynx is nasal tamponade with multiple strips of gauze up to 10 cm long according to Beninghouse. They are stacked on top of each other, starting from the bottom of the vestibule of the nose.
Rice. 18-1. Anterior (a) and posterior (b) nasal cavity tamponade
If anterior tamponade is ineffective, posterior tamponade is performed. To do this, a thin rubber catheter is inserted along the lower nasal passage into the nasopharynx. After the end of the catheter appears in the oropharynx, it is grabbed with tweezers and a pre-prepared special nasopharyngeal swab is tied to it with two threads. After this, the catheter with threads is removed from the nose, and the tampon is inserted behind the soft palate with a finger, where it is pressed tightly into the choanae. The threads removed from the nose are pulled tightly, and then anterior nasal tamponade is additionally performed. Both threads are tied over a gauze roll at the entrance to the nose (see Fig. 18-1 b). The end of the third thread left in the mouth is wrapped around the ear or attached to the cheek with an adhesive plaster (for subsequent removal of the tampon).
When bleeding from the nose, a posterior tampon is needed to successfully perform the tightest anterior tamponade and more reliably delineate the nasopharynx. It is necessarily used to stop bleeding from the posterior ends of the nasal turbinates and those arising from tumors of the posterior parts of the nasal cavity. Posterior tamponade is difficult for patients to tolerate. It should be done after preliminary premedication with atropine and promedol (omnopon). It is necessary to ensure that the posterior tampon is behind the uvula, otherwise there is a risk of developing necrosis of the uvula from pressure.
The optimal period for tamponade, when a durable blood clot forms in the damaged vessel, is 4-6 days (Nevsky B.N., 1983). To prevent the development of infection, tampons placed in the nose are repeatedly impregnated with solutions of antibiotics or antiseptics.
For nasal tamponade, rubber pneumatic cylinders designed by Mezrin, Lapchenko and Nevsky, Mazing (Fig. 18-2.), etc. are also used. They ensure the tightness of the nasal cavity and nasopharynx during both posterior and anterior tamponade, and are easier to tolerate by patients. Air can be periodically released from the pneumatic cylinder, thereby giving “rest” to the nasal mucosa and preventing the possibility of its necrosis.
Rice. 18-2. Masinga pneumatic tampon and nasal tamponade with its help
When nosebleeds occur, local fibrinolysis is activated with lysis of the resulting blood clots. In this regard, regardless of the cause of nosebleeds, it is recommended in all cases to soak tampons with a 5% solution of e-aminocaproic acid. For bleeding disorders, it is advisable to apply thrombin, fibrin film and hemostatic sponge topically.
For hypertension, if blood pressure is high, 10 ml of a 25% solution of magnesium sulfate is injected intramuscularly, papaverine and dibazole are prescribed (drugs that increase blood clotting are contraindicated).
For thromboplastic bleeding, prednisolone may be prescribed.
If blood clotting disorders are detected, appropriate pathogenetic transfusion therapy is carried out.
If the cause of nosebleeds is leukemia, then a hemostatic effect can be achieved with the help of corticosteroid drugs, especially prednisolone, and for tamponade it is best to use oxidized cellulose in the form of gauze. For such patients, it is advisable to prescribe a transfusion of platelet concentrate, administration of iron supplements, Vicasol, rutin, gelatin, calcium chloride.
Often the cause of persistent nosebleeds is Osler's disease - hereditary hemorrhagic telangiectasias of the skin and mucous membranes. During rhinoscopy, performed after anemization, slightly elevated and elevating the epithelium are visible pinpoint angiomatous dilations of the vessels. Treatment of Osler's disease is mainly symptomatic.
In case of severe bleeding, arteries are ligated or embolized: the external carotid, internal maxillary or ethmoidal arteries, and in exceptional cases - the common carotid. The external carotid artery is most often ligated. However, unilateral ligation of the external carotid artery is not the optimal way to stop epistaxis. It can continue through anastomoses. In this regard, it is more advisable to interrupt the blood flow closer to the site of bleeding, so ligation of the internal maxillary artery gives the best effect.
Ligation of the external carotid and maxillary arteries is effective only if the source of bleeding is located below the middle concha. If it is located higher, then bleeding may occur from the ethmoid arteries belonging to the internal carotid artery system.
The ethmoidal arteries are most easily identified and ligated in the orbit using the Killian incision approach used in external ethmoidectomy.
Another way to stop bleeding from the ethmoidal arteries is ethmoidectomy, which can be performed internally or externally. In both cases, it is more advisable to perform the operation under intubation anesthesia in the presence of a sealing nasopharyngeal tampon.
To stop nosebleeds from the external carotid artery system, embolization of its terminal branches has recently been successfully used, in particular for vascular tumors of the nose, paranasal sinuses, nasopharynx and idiopathic bleeding. However, it must be taken into account that when using this method there is a risk of complications (brain or lung infarctions, necrosis, tissue infection, etc.). Currently, it is optimal to detect the source of bleeding under endoscopic control, after which it is stopped.
Previous7Next
Date added: 2016-06-05; views: 3268; ORDER A WORK WRITING
Similar articles:
Diagnosis of nosebleeds
Correct diagnosis helps to localize the process, find out its cause and choose the optimal treatment method. Such activities are carried out only in the office of an otolaryngologist and usually consist of several stages.
Analysis of the patient's history and complaints:
- When did the first complaints appear?
- Was there a previous injury to the nose?
- Is there a history of concomitant diseases?
General inspection includes:
- determination of the condition of the skin and mucous membranes;
- measurement of pulse rate and pressure indicators.
Rhinoscopy:
- examination of the nasal area and determination of the location of the local process;
- determines whether blood flows from one nostril or through both nasal passages;
Pharyngoscopy:
- assesses the condition of the mucous surface of the pharynx;
Blood test:
- reflects the volume of blood loss and the functioning of the blood coagulation system;
- The amount of iron in the serum helps to assess the degree of possible anemia.
Treatment of nosebleeds
It is not always possible to stop a nosebleed on your own. In this case, drug treatment may be used. In this case, the patient is prescribed hemostatic drugs intravenously/intramuscularly or orally. They are chosen depending on the severity of the bleeding. For minor and moderate epistaxis, you should take 1-2 teaspoons of 10% calcium chloride. It enhances the effect of hemostatic drugs, improves the contractility of vascular walls and reduces their permeability.
Doctors prescribe the following drugs to stop epistaxis:
- Sodium ethamsylate solution 12.5% (dicinone), which enhances platelet function and helps stop bleeding. It does not affect blood clotting, so it is prescribed for a long time. It is used orally or intravenously;
- Vikasol, which enhances the effect of hemostatic drugs, but it cannot be used for more than 3-4 days. This drug is administered intramuscularly;
- Aminocaproic acid, which reduces processes leading to blood thinning. It is administered intravenously (more than 60 drops per minute). This drug is contraindicated in DIC (intravascular coagulation disorder) because it increases blood clotting.
The patient should also take vitamins C and K. For severe nosebleeds, transfusions of blood components are used. The patient is injected with at least 500 ml of fresh plasma, which has a hemostatic effect. For nosebleeds that persist for a long time, surgical treatment methods can be used.
Anterior tamponade
Anterior tamponade, which stops bleeding from the anterior nasal cavity, is performed as follows:
- During the procedure, the nasal area is anesthetized with an aerosol 10% lidocaine solution or instillation of 2% dicaine.
- A gauze swab (turunda) up to 20 cm long and up to 1.5 cm wide is inserted into the nostril.
- Before insertion into the nose, the turunda is moistened with 3% hydrogen peroxide, which accelerates the formation of a blood clot, or a 5% solution of aminocaproic acid, which has a hemostatic effect.
- Turunda can also be moistened with thrombin or hemophobin.
- After inserting the tampon, a sling-shaped bandage is applied to the nose.
- Leave the turunda in the nose for 1-2 days, injecting aminocaproic acid into the tampon daily. In especially severe cases, turundas are left in the nose for 6-7 days.
- Before removing the tampon, 3% hydrogen peroxide is injected into it to make it moist and easier to remove.
Posterior tamponade
Posterior tamponade, necessary for severe bleeding from the posterior nasal cavity, is performed as follows:
- For this procedure, prepare sterile swabs from folded gauze. Their size should be 2.5x2 cm.
- The tampon is tied with two silk threads 20 cm long, crosswise. One of the four ends of the threads is cut off.
- Before the procedure, intramuscular anesthesia is performed with a lytic mixture consisting of aqueous solutions of 1 ml of 1% promedol, 2 ml of 50% analgin, 1 ml of 2% diphenhydramine.
- The procedure begins by inserting a thin rubber catheter into the bleeding nostril. It is injected until it comes out through the nasopharynx into the pharynx.
- Then, using forceps or tweezers, the catheter is pulled out through the mouth.
- A tampon is tied to the end of the catheter and pulled into the nasal cavity until it stops at the choanae (inner nasal openings).
- The tampon is held in place by two stretched strings that extend from the nasal opening.
- The third thread is removed from the mouth. It is glued to the cheek with an adhesive plaster.
- For reliability, the posterior tamponade is supplemented with the anterior one.
- Tampons are left in the nose for 1-2 days. In severe cases - for 6-7 days. The patient should take antibiotics and sulfa drugs to prevent infectious diseases and rhinogenic sepsis.
- Tampons are removed using silk threads.
Surgery
Surgery is used in 5-17% of cases of persistent extensive nosebleeds.
In this case, it is possible to influence the nasal cavity using the following methods:
In case of long-term continuous nosebleeds, cauterization of the nasal mucosa is performed in a hospital setting. For this, a wide variety of cauterizing agents are used: chromic, trichloroacetic, lactic acid, silver nitrate solution, alum, tannin, zinc salts; they also resort to galvanocaustics or surgical diathermy. All these remedies differ from each other in the degree and depth of cauterization. A scar subsequently forms at the cauterization site.
Recently, ultrasonic disintegration, laser therapy and cryogenic treatment with liquid nitrogen have been successfully used for nosebleeds. Cold exposure can be carried out using a one- or two-cycle method.
In severe cases, general measures are taken. Their purpose is to increase blood clotting and constrict peripheral blood vessels. Great importance is attached to agents acting on the anticoagulation system of the blood. It is advisable to use a 10% solution of calcium chloride, vitamin K (Vicasol 0.015 g), rutin, and corticosteroids.
Oxygen therapy can be used to stop nosebleeds. If you give oxygen from an oxygen bag to the patient while breathing calmly and evenly, the bleeding stops quite quickly. Apparently, such an event prevents or eliminates blood stagnation and has a calming effect.
The patient is prohibited from talking, any movement, or reading.
If the nosebleeds cannot be stopped by the listed measures, you should resort to ligation of the afferent blood vessels along their length. If after ligating a blood vessel on one side the bleeding does not stop, then it is necessary to ligate it on the other side. In some cases, only such a measure of assistance can prevent death. These activities are carried out in specialized otorhinolaryngological or general surgical departments of hospitals.
If the nosebleed is significant, you should temporarily refrain from eating. There is no need to give hot food and especially drink hot drinks such as strong tea and cocoa, as they can increase blood pressure and dilate the lumen of blood vessels. Food rich in proteins is recommended (taking into account sensitivity to it): cottage cheese, lightly fried liver, concentrated chicken broth, as well as fresh vegetables, fruits, juices, vitamins.
Various ways to stop bleeding and prevent the development of possible reoccurrences are the tactics for treating nasal bleeding. Prevention of relapses is associated with the treatment of diseases against which they can occur.
Methods of stopping depend on the location and severity of the process. Epistaxis from the anterior region can be stopped independently. To do this, it is enough to lightly press the corresponding wing of the nose against the septum, and then insert a tampon with a hemostatic agent. And yet, despite the majority of successful outcomes, in case of nosebleeds it is necessary to consult an otolaryngologist. This is especially important when relapses and severe blood loss are observed.
Stopping nosebleeds can be done in several ways:
- Mechanical involves performing anterior or posterior packing, during which hemostatic sponges or balloons are installed in the nasal passages;
- Chemical stopping is performed using a variety of chemical materials;
- The physical method involves the local action of different temperatures, as well as sealing of vessels using an electrocoagulator;
- Pharmacological stopping is carried out by prescribing medications that improve blood clotting;
- The operative, surgical method is indicated for recurrent and severe processes with severe blood loss. It can be carried out by cutting, ligating arteries and vessels, as well as using embolization.
- Mixed combines all possible options.
If the measures taken do not stop the bleeding within 15 minutes, it is necessary to call an ambulance and hospitalize the child in the ENT department, where specialized medical care will be provided.
Indications for urgently calling an ambulance are as follows:
- nasal injury in a child;
- intense bleeding and the threat of massive blood loss;
- discharge of clear fluid with blood after a head injury (possible fracture of the base of the skull);
- diabetes;
- hemophilia or other pathology of the blood coagulation system;
- bleeding developed due to the use of heparin, ibuprofen, aspirin, indomethacin or other drugs that impair blood clotting;
- resumption of bleeding after it stops;
- bleeding due to high blood pressure in children;
- vomiting blood or foamy blood coming from the nose;
- loss of consciousness due to bleeding.
In a hospital, if there is bleeding from the anterior part of the nose, it can be stopped by coagulating (cauterizing) the bleeding vessel with a laser, liquid nitrogen or electricity (electrocoagulation).
Indications for vascular coagulation:
Nose bleed
Bleeding from the nose is a symptom of a local nasal lesion or a general disease. The source of nosebleeds can be in different parts of the nose, but the most common bleeding area is the anterior inferior part of the nasal septum (Kiesselbach's place). The most common cause of nosebleeds is trauma, which can be mild, causing minor bleeding, or severe, causing damage to facial tissue that can cause profuse, life-threatening bleeding.
Local causes of nosebleeds can be surgical interventions, neoplasms, syphilitic or tuberculous ulcers.
Common causes of nosebleeds are diseases of the vascular system and blood (hypertension, heart defects, emphysema, liver disease, spleen disease).
Severe nosebleeds occur with hemorrhagic diathesis (hemophilia, hemorrhagic thrombasthenia, Werlhoff's disease, hemorrhagic vasculitis, etc.). The causes of nosebleeds in these diseases are heterogeneous: in some cases the system of blood clotting factors is disrupted, in others the vascular wall is damaged. Diseases of the hematopoietic organs (leukemia, reticulosis, etc.) can also be accompanied by nosebleeds.
Various other factors may play a role in the occurrence of nosebleeds:
- hypo- and vitamin deficiencies;
- low atmospheric pressure;
- great physical stress;
- overheating of the body, etc.
In some patients, bleeding from the nose begins unexpectedly, others note prodromal phenomena - headache, tinnitus, dizziness, itching or tickling in the nose. It must be borne in mind that blood into the nose can flow from other parts of the upper respiratory tract - the pharynx, larynx, trachea, lung, and in rare cases from the middle ear through the auditory tube. With nosebleeds, the blood is clean and of normal appearance; its flow down the back wall of the throat is clearly visible, especially when the head is thrown back.
Usually the bleeding occurs from one side of the nose, but sometimes the blood flows into the healthy half of the nose. There are:
- minor;
- moderate;
- severe nosebleeds.
Minor bleeding , as a rule, occurs from the Kisselbach area: blood in a volume of several ml is released in drops for some time. Such bleeding often stops on its own. Outwardly harmless, but often repeated, long-term, minor discharge of blood from the nose can have a particularly negative effect on a young body.
Moderate nosebleeds are characterized by more abundant bleeding (within 200 ml). In this case, the change in hemodynamics is within normal limits.
In children and weakened adults, external bleeding often does not give a complete picture of the true blood loss, since some of the blood flows into the pharynx and is swallowed. Insufficient assessment of this is fraught with serious complications: in such cases, profuse bloody vomiting usually occurs, blood pressure drops, and the pulse quickens.
With severe nosebleeds, the volume of blood lost per day exceeds 200 ml, sometimes reaching 1 liter or more. Such bleeding poses an immediate threat to life. Post-traumatic nosebleeds are often characterized not only by profuseness, but also by recurrence after several days, and possibly even weeks. Large blood loss with severe bleeding causes a drop in blood pressure, increased heart rate, severe general weakness, and sweating.
Treatment of nosebleeds
The simplest method of stopping nosebleeds is to insert a ball of sterile cotton wool or gauze soaked in a solution of hydrogen peroxide into the anterior section of the bleeding half of the nose for 15-20 minutes. Stopping recurrent nosebleeds, as well as prolonged, massive bleeding, is carried out in a hospital using appropriate methods, such as cauterization of bleeding vessels, anterior and posterior nasal tamponade, and, if necessary, replenishing the volume of circulating blood, red blood cells, and flooding the body.
IMPORTANT!!! We must remember that repeated or recurrent nosebleeds are most often symptoms of some disease. Only a doctor can understand the causes of this condition, so the presence of bleeding is a mandatory indication for seeking medical help.
← Back
First aid for epistaxis
You should not throw your head back.
Against! It is necessary to lean forward slightly and firmly press the wings of the nose to the nasal septum with your fingers. If nosebleeds occur, you should:
- Calm the child, because excitement from the sight of blood will cause increased heart rate and increased blood pressure, which will increase bleeding and increase blood loss.
- Place the child in a sitting or reclining position, with his head slightly lowered down, so that the blood does not flow into the respiratory tract or esophagus, but flows out of the nostrils. In a horizontal (lying) position, the flow of blood to the head will increase and the bleeding will intensify.
Scope and tactics of diagnostic measures
Find out complaints , collect anamnesis of the disease, find out the possible cause of nosebleeds.
Local causes leading to nosebleeds:
- Injuries: injury to the nasal mucosa, fracture of the nasal bones and/or facial bones.
- Foreign bodies in the nasal cavity.
- Inflammatory, atrophic diseases of the nasal mucosa.
- Local exposure to chemicals.
- Neoplasms of the nasal cavity and nasopharynx.
- The cause has not been determined.
General causes leading to nosebleeds:
- Diseases of the cardiovascular system (arterial hypertension, heart defects and vascular abnormalities with increased blood pressure in the vessels of the head and neck, atherosclerosis, liver disease).
- Coagulopathies, hemorrhagic diathesis, diseases of the blood system, hypo- and avitaminosis, radiation sickness.
- Intoxication with heavy metals, mercury, phosphorus, chromium.
- Hyperthermia (acute infectious diseases, heat and sunstroke, overheating).
- Sepsis.
- With sudden changes in barometric pressure (pathological syndromes in flight, diving, mountaineering practice).
- Hormonal imbalance (juvenile and vicarious bleeding).
Carry out an objective examination, pay attention to signs of nosebleeds:
- visually determined flow of non-foaming blood from the lumen of the nostrils and/or flow of blood along the back wall of the pharynx.
Assess the amount of blood loss.
Estimate:
- level of consciousness;
- breathing quality;
- hemodynamic parameters;
- color and moisture of the skin.
Assess the possibility of complications :
- hemorrhagic shock;
- fainting;
- posthemorrhagic anemia.
Carry out differential diagnosis , exclude:
- bleeding from the respiratory tract: scarlet foamy blood when coughing, hemoptysis.
- bleeding from the veins of the esophagus, characteristic anamnesis and examination data.
Issue an “EMS Call Card”.
Monitoring the general condition of the patient, respiratory rate, heart rate, pulse, blood pressure, thermometry, pulse oximetry.
Complications
The consequences of the pathology in question depend on its frequency and severity. It was previously mentioned that weak and minor bleeding may stop spontaneously. They are not a danger to human life. But abundant and repeated ones can end sadly and lead to serious hemorrhagic shock. It is manifested by lethargy, a sharp drop in blood pressure, and a weak, barely perceptible pulse. This condition is a reason to immediately call an ambulance.
Preventing nosebleeds
Preventive measures depend on the etiology of the disease. People suffering from frequent epistaxis should first of all know the reasons for their occurrence. Are they associated with a rise in blood pressure or not? Do you have a history of a general illness that is associated with nasal bleeding? Have there been any injuries to the nasal mucosa?
To prevent bleeding, excessive physical activity should be avoided. It is necessary to eat a healthy and balanced diet and drink enough fluids per day. The air in apartments and work areas should not be allowed to dry out; if possible, use humidifiers and air ionizers. It is very important to promptly treat acute inflammation of the paranasal sinuses and nose. It is worth paying attention to the quality and shape of the sleeping pillow; it is best to use an orthopedic model. It is undesirable to allow damage to the nasal mucosa. Periodically you need to moisturize it with oil solutions of vitamin A and E.
In case of frequent and seemingly causeless nasal bleeding, examination by a hematologist, endocrinologist, or neurologist is mandatory. When taking medications that change blood clotting, blood levels should be monitored regularly. It is necessary to carry out annual prevention of acute respiratory viral infection, do not forget about hardening and vitamin therapy. And, of course, one of the important preventive measures is consultation with a qualified ENT doctor.
Emergency care for nosebleeds
Both children and adults need to know the rules of first aid for the described syndrome - this way they can help themselves, and a simple passer-by or neighbors, acquaintances and colleagues.
What to do if you have anterior nosebleeds
First of all, you need to sit up or lay down the victim (in a lying position, the head must be slightly raised).
Please note: you should not raise your head too much, as this may lead to swallowing blood.
Next you need to apply one or two methods:
- 3% hydrogen peroxide;
- vasoconstrictor nasal drops (for example, Naphthyzin).
With these remedies, you need to moisten a cotton swab and insert it into the nostril where the blood is coming from (or both), squeeze the nasal passage with the swab a little with your fingers and remain in this position for a maximum of 15 minutes. You can apply cold to the bridge of your nose as additional help - even ice from the refrigerator will do.
If you don’t have a first aid kit at hand, you can quickly stop mild bleeding from the front nose with a regular handkerchief - moisten it in water and apply it to the bridge of your nose.
Important: if bleeding from the nose continues after the measures taken and blood flows out in a stream, with clots, you should urgently seek medical help.
What to do if you have a posterior nosebleed
In this case, you cannot do without the help of specialists, so you need to call an ambulance and go (or send the victim) to the hospital. What can doctors do in a medical facility?
Firstly, specialists direct their actions to stop bleeding. To do this, tampons soaked in specific medications are inserted into the nasal passages. Such tamponade can last more than 1 day. At the same time, doctors can inject hemostatic agents, which will help speed up the process of restoring normal functioning of the nose.
Secondly, if the above measures do not produce any effect within 2 days, then surgical intervention is prescribed - surgeons will stop the bleeding using coagulation, restoring the integrity of the damaged vessel. There is nothing terrible about such an operation - specialists work with ultra-modern equipment and there is no need to open the nose.
Thirdly, after emergency assistance is provided, a full examination of the patient will be carried out, the causes of nosebleeds will be identified and specific medications will be prescribed (for example, to strengthen the walls of blood vessels). It is much easier to undergo a course of therapy and then just follow the recommendations of your doctor than to deal with blood loss every time.
Please note: all of the above activities are carried out in medical institutions only for those patients who have been seen by a doctor without visible signs of deterioration in health. In all other cases, an emergency examination of the patient is carried out - ultrasound and x-ray examinations will enable doctors to understand what is happening in the patient’s body.
Many people try to cope with prolonged nosebleeds on their own, using traditional recipes. Please note that this behavior is fraught with serious consequences:
- visible bleeding may become less, in fact the blood simply flows down the throat into the esophagus and stomach;
- if the described syndrome is associated with a nasal injury, then stopping the bleeding may mean a fracture of the distant bones of the nasal sinuses, the penetration of their fragments into the skull;
- the loss of blood is so great that it can end very sadly for the patient.
Nosebleeds most often turn out to be a harmless syndrome that even a child can cope with. But you should be attentive to your own health and if the syndrome recurs (more than once every two months), you need to consult a doctor for a full examination. Even if children have bleeding and it is not intense, then consulting a specialist will not hurt - this syndrome may indicate banal fragility of blood vessels, but it can also be a sign of serious pathologies of internal organs.
Tsygankova Yana Aleksandrovna, medical observer, therapist of the highest qualification category.
17, total, today
( 49 votes, average: 4.37 out of 5)
Atherosclerosis: symptoms, diagnosis, treatment
Varicose veins of the lower extremities: causes, complications, prevention