The frontal sinuses are an integral part of the paranasal cavities. This area is responsible for several functions, but the main task is to protect the body and normalize the pressure of the respiratory tract.
It is important to know that the frontal sinuses are located in close proximity to the brain, so inflammation in this area is especially dangerous. It is known that almost fifteen percent of people suffer from diseases in this area.
Peculiarities
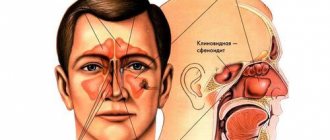
The frontal sinus or frontal sinus is a cavity in the bone located behind the brow ridge, shaped like an irregular pyramid with smoothed corners. Its sides are: the outer wall of the frontal bone in front, the upper wall of the orbit below, the back wall is the inner side of the frontal bone, bordering the frontal lobe of the brain, the inner wall is, in fact, the intersinus septum. The norm is that they are asymmetrical, that is, the partition is always slanted to the side.
The inside of the frontal sinus is lined with a mucous membrane containing goblet cells that produce secretions. The latter moisturizes the nasal cavity, protects its mucous membrane from damage and various infections.
A developmental anomaly is considered to be slit-like communications between the sinuses and surrounding tissues. They are called dehiscences. For example:
- Communication of the ethmoidal labyrinth with all sinuses.
- Holes in the lateral wall of the sinus. They bring its mucosa into contact with the meningeal membrane and the optic nerve, cavernous sinus and internal carotid artery.
- Reducing the thickness of the wall of the sphenoid sinus. This anomaly promotes contact with the abducens and trochlear, oculomotor and trigeminal nerves.
Physiological features
There are unfilled spaces in the facial bones of every person's skull. These are the sinuses of the nose, which in medicine are called paranasal or paranasal.
Air passes through them, so they are connected to the nose. Depending on the location of the sinuses, they form groups:
- the maxillary cavities are paired and are located in the upper jaw; there is a frontal cavity in the frontal bone; in the main bone of the skull there is a wedge-shaped cavity; The ethmoid cavity is formed from parts of the ethmoid bone.
The paranasal sinuses perform the following functions:
- breathing, because they are the ones who moisturize, warm and purify the inhaled air before it enters the lungs. This makes it clear why impaired nasal breathing generally worsens the well-being of the entire body; protection, since they are the ones who hold back coarse particles. So, when such particles get on the mucous membrane, it becomes irritated and the person sneezes, thereby clearing the nasal passages; sense of smell, special epithelial tissue helps detect odors; The paranasal sinuses take part in the formation of the timbre of the voice.
The frontal sinus is divided into 2 parts, and its sections are pneumatized in different ways. The same thing happens with the sphenoid sinus, which also has 2 parts and their pneumatization is different.
The paranasal sinuses are examined externally by a doctor, when the nasal and oral cavity and their swelling are visible. Upon palpation, you can notice pain in the patient. However, a deep examination can only be carried out using rhinoscopy.
A more complex diagnostic technique is probing, which is carried out either through the frontal or through the sphenoid cavity.
The frontal sinus or frontal sinus is a cavity in the bone located behind the brow ridge, shaped like an irregular pyramid with smoothed corners. Its sides are: the outer wall of the frontal bone in front, the upper wall of the orbit below, the back wall is the inner side of the frontal bone, bordering the frontal lobe of the brain, the inner wall is, in fact, the intersinus septum. The norm is that they are asymmetrical, that is, the partition is always slanted to the side.
A developmental anomaly is considered to be slit-like communications between the sinuses and surrounding tissues. They are called dehiscences. For example:
- Communication of the ethmoidal labyrinth with all sinuses.
- Holes in the lateral wall of the sinus. They bring its mucosa into contact with the meningeal membrane and the optic nerve, cavernous sinus and internal carotid artery.
- Reducing the thickness of the wall of the sphenoid sinus. This anomaly promotes contact with the abducens and trochlear, oculomotor and trigeminal nerves.
The paranasal sinuses are represented by cavities internally covered with epithelial tissue. Most of them are located in the bones of the facial skull or within the anterior cranial fossa.
Another important function is to humidify and warm the air while it is in the sinuses. Also, the sinuses themselves perform a resonator function for the voice - they provide its tonality, sonority and individual coloring
Thus, they are quite important structures of the human body.
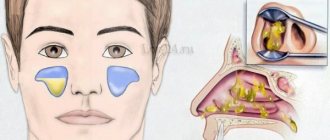
The frontal sinuses are located directly in the thickness of the frontal bone posterior to the superciliary arches. They communicate with the nasal cavity through the middle meatus via the frontonasal canal.
A characteristic feature of the frontal sinus is that at birth this sinus is absent - it develops only by the 7-8th year of life, reaching its maximum development by puberty - for boys - 13-14, for girls - 12-13 years.
Basic definitions
It is also necessary to consider the basic concepts. Hypoplasia is a varying degree of underdevelopment of some anatomical unit, up to its complete absence. This is a congenital defect of the above cavity, which is a consequence of incorrect resorption of cancellous bone tissue.
There are several types of hypoplasia. Aplasia is a defect when development has not yet begun, while agenesis is when it began, but stopped at a certain stage. Atresia is the complete absence of an opening.
Classification of hypoplasia of the frontal sinuses
There is congenital hypoplasia, acquired or secondary.
A doctor can diagnose a unilateral form of pathology. For example, there is hypoplasia of the frontal sinus on the right. What this is is already clear from the name. Of course, this is not the only scenario. Hypoplasia of the left frontal sinus also occurs with the same frequency. The doctor will tell you what it is if he discovers such an anomaly. It is characterized by obligatory facial asymmetry on the affected side. There may also be some defect or reduction in the size of the sinus on the opposite side. The diagnostic puncture method in this case will be the most informative.
There is also bilateral hypoplasia and multilocular (trabecular).
Diagnostics
https://www.youtube.com/watch?v=BQLf2zVZjlw
The symptoms of diseases of the frontal sinuses, be it frontal sinusitis or a cyst, are the same. The only difference is that a cyst, if it is small in size, may not show any signs at all for quite a long time. In addition, minor neoplasms are not always detected during routine examinations by an ENT specialist.
The main symptoms of frontal sinus disease are:
- pain in the forehead, which intensifies with pressure and fatigue;
- purulent nasal discharge, often odorless;
- disruption of normal breathing, usually from the affected cavity;
- swelling and redness of the skin at the site of the inflamed sinus;
- a sharp increase in body temperature;
- general weakness.
Epidemiology and etiology of the disease
As we have already said, underdevelopment of the sinuses can be unilateral or bilateral. 3-5% of people in the world do not have them at all (one or two). In 71% of cases, sinuses are absent on one side, in 29% - on both sides. In 45% of cases, hypoplasia is observed, in 55% - complete aplasia. Multilocular sinuses are quite common - this is called trabecular hypoplasia. This pathology is typical for men.
Hypoplasia of the frontal sinuses develops as a result of exposure to unfavorable factors on the fetus: oligohydramnios, injuries, fever, chemicals, including drugs, alcohol and nicotine, maternal diseases, TORCH infections, intrauterine infections, birth injuries in the facial area.
Clinical anatomy of the paranasal sinuses
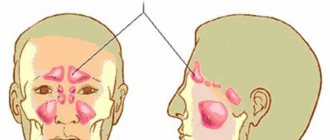
The paranasal sinuses are air cavities located around the nasal cavity and communicating with it through the outlet openings or ducts. There are four pairs of sinuses: maxillary, frontal, ethmoidal labyrinth and sphenoid (main). The clinic distinguishes between the anterior sinuses (maxillary, frontal and anterior and middle ethmoid) and posterior (posterior cells of the ethmoid bone and sphenoid). This division is convenient from a diagnostic standpoint, since the anterior sinuses open into the middle nasal passage, and the posterior sinuses open into the upper nasal passage.
The maxillary sinus , (also known as the maxillary sinus) located in the body of the maxillary bone, is an irregularly shaped pyramid measuring from 15 to 20 cm3. The anterior or facial wall of the sinus has a depression called the canine fossa. The sinus is usually opened in this area. The medial wall is the lateral wall of the nasal cavity and contains a natural outlet in the area of the middle nasal meatus. It is located almost under the roof of the sinus, which impedes the outflow of contents and contributes to the development of congestive inflammatory processes. The upper wall of the sinus simultaneously represents the lower wall of the orbit. It is quite thin, often has bone nonfusion, which contributes to the development of intraorbital complications. The lower wall is formed by the alveolar process of the maxilla and usually occupies the space from the second premolar to the second molar. The low position of the sinus floor promotes close proximity of the tooth roots to the sinus cavity. In some cases, the apices of the roots of the teeth stand in the lumen of the sinus and are only covered by the mucous membrane, which can contribute to the development of odontogenic infection of the sinus, the entry of filling material into the sinus cavity, or the formation of a persistent perforation during tooth extraction. The posterior wall of the sinus is thick and borders the cells of the ethmoidal labyrinth and the sphenoid sinus.
The frontal sinus is located in the thickness of the frontal bone and has four walls: the lower orbital - the thinnest, the anterior - the thickest up to 5-8 mm, the posterior, separating the sinus from the anterior cranial fossa, and the internal - septum. The frontal sinus communicates with the nasal cavity through a thin winding canal that opens into the anterior section of the middle meatus. The size of the sinus ranges from 3 to 5 cm3, and in 10-15% of cases it may be absent.
The ethmoid labyrinth is located between the orbit and the nasal cavity and consists of 5-20 air cells, each of which has its own outlet openings into the nasal cavity. There are three groups of cells: anterior and middle, opening into the middle nasal meatus, and posterior, opening into the upper nasal meatus.
The sphenoid, or main, sinus is located in the body of the sphenoid bone, divided by a septum into two halves, which have independent access to the area of the upper nasal passage. Near the sphenoid sinus are the cavernous sinus, carotid artery, optic chiasm, and pituitary gland. As a result, the inflammatory process of the sphenoid sinus poses a serious danger.
The blood supply to the paranasal sinuses occurs through the branches of the external and internal carotid arteries. The veins of the maxillary sinus form numerous anastomoses with the veins of the orbit, nose, and sinuses of the dura mater.
Lymphatic vessels are closely connected with the vessels of the nasal cavity, the vessels of the teeth, the retropharyngeal and deep cervical lymph nodes.
Innervation is carried out by the first and second branches of the trigeminal nerve.
Features of the structure of the paranasal sinuses in childhood
Newborns have only two sinuses: the maxillary sinus and the ethmoidal labyrinth.
The maxillary sinus is a fold of mucous membrane about 1 cm long at the inner corner of the orbit; laterally, under the lower wall of the orbit, there are two rows of rudiments of milk and permanent teeth. By the end of the first year of life, the sinus acquires a rounded shape. By the age of 6-7 years, the teeth gradually take their position, and the sinus becomes multifaceted. In early childhood, the canine is located closest to the sinus; at 6 years, two premolars and a molar are located. By the age of 12, the volume of the sinus increases and the topography approaches the norm of an adult.
The cells of the ethmoid labyrinth in newborns are in their infancy and are fully developed by 14-16 years.
The frontal and sphenoid sinuses are absent in newborns and begin to form from 3-4 years of age. The frontal sinuses develop from the anterior cells of the ethmoidal labyrinth and by the age of 6 have a volume of about 1 cm3. The sphenoid sinuses are formed from cells of the ethmoid labyrinth located in the body of the sphenoid bone. The final development of the sinuses ends by 25-30 years.
Pathogenesis of frontal sinus hypoplasia
The formation of frontal sinuses is a genetically programmed process. Every child is born without them, that is, a newborn baby does not have them at all. The frontal sinuses normally begin to develop at about 7-8 years of age and by the age of 25 this process ends. Their cavity in an eight-year-old child is a maximum of 0.7 cm 3, and in adults it reaches 7 milliliters.
Functions of the frontal sinus or frontal sinus:
- reducing the mass of the skull, making it lighter;
- protection of the brain from injury, a kind of shock absorption;
- acoustic function, formation of a characteristic voice timbre;
- individuality of facial features;
- moisturizing the mucous membranes of the nasal cavity.
Agenesis or atresia of the frontal sinuses can also be acquired. Such hypoplasia is essentially secondary sclerosis. This occurs as a result of past infections - frontal sinusitis, pansinusitis, or injuries to the facial area. Their consequences are regression of cavity development and bone compaction.
Causes and course of the disease
The cause of acute frontal sinusitis may be acute rhinitis or ethmoiditis (inflammation of the mucous membrane of the ethmoid labyrinth cells), acute respiratory diseases, hypothermia, or a general viral infection.
The causes of acute frontal sinusitis may be:
- anatomically narrow frontonasal anastomosis;
- difficulty in the outflow of secretions from the frontal sinus;
- swelling of the mucous membrane of the nasal cavity and frontal sinus.
Morphological changes in acute frontal sinusitis are similar to the changes that occur in maxillary sinusitis.
Methods for identifying this pathology
This includes the following:
- X-ray examination;
- Magnetic resonance imaging;
- ultrasonography;
- CT scan;
- diagnostic puncture.
An X-ray can show a decrease in the transparency of the sinus, which is often misdiagnosed as sinusitis, and the person is subjected to unnecessary treatment. Doctors consider this method unreliable.
According to experts, tomography today is the only method that reliably makes it possible to determine malformations and anatomical variants of the development of structures, including those forming the ostiomeatal complex. Using computed tomography, it is possible to determine which sinus is smaller, its bony walls are pressed into the sinus or thickened, but retain smooth and clear contours, and the nasal cavity is expanded or not.
Let's understand the terms
This includes the following:
- X-ray examination;
- Magnetic resonance imaging;
- ultrasonography;
- CT scan;
- diagnostic puncture.
An X-ray can show a decrease in the transparency of the sinus, which is often misdiagnosed as sinusitis, and the person is subjected to unnecessary treatment. Doctors consider this method unreliable.
According to experts, tomography today is the only method that reliably makes it possible to determine malformations and anatomical variants of the development of structures, including those forming the ostiomeatal complex. Using computed tomography, it is possible to determine which sinus is smaller, its bony walls are pressed into the sinus or thickened, but retain smooth and clear contours, and the nasal cavity is expanded or not.
To indicate the complete absence of sinuses or a delay in their normal development, doctors use different (but essentially identical) terms and designations:
- aplasia;
- atresia;
- hypoplasia;
- agenesis and so on.
In some clinical cases, regressive development of the sinuses is possible when an inflammatory process occurs and affects the already developed frontal sinuses. Quite often I use agenesis and aplasia as synonyms, denoting the same phenomenon.
If we take into account the characteristic features of the formation of the frontal sinuses, then it makes sense to use the terms aplasia and agenesis. The first word denotes the complete absence of the process of formation and development (hypoplasia of the frontal sinuses). The second is that there is a delay in the process of organ formation that has begun.
Symptoms and treatment
There are no symptoms as such, and it does not matter whether there is hypoplasia of the right frontal sinus or the left. In some cases, a person may experience mild discomfort. There may be unpleasant sensations in the bridge of the nose and above, in the corner of the eye, nasal congestion, and lacrimation. Usually this is a sign of regressive agenesis, that is, secondary, developing as a result of changes in the mucous membrane after an infection.
According to scientists, a congenital anomaly can be considered as a variant of development and even as a variant of the norm. It is detected incidentally and does not require any treatment or observation. On the contrary, under no circumstances should hypoplasia be confused with the inflammatory process and sinus cysts. Since in this case there is no need to treat hypoplasia of the frontal sinuses, you can only engage in prevention.
This is done by eliminating harmful factors affecting the fetus. During pregnancy planning, all maternal diseases should be treated, especially infections and endocrine problems. It is necessary to exclude all chemical attacks on the fetus: for example, you should change jobs that are harmful to health.
Consequences of frontal sinus hypoplasia
As a result of recent clinical studies, it has become clear that hypoplasia of the frontal sinus is not the cause and does not at all affect the occurrence of inflammation of the mucous membranes of the paranasal sinuses or sinuses, which is called sinusitis.
This is frontal sinusitis, sinusitis, ethmoiditis or inflammation of the mucous membranes of all sinuses at once (pansinusitis). Such diseases are complications of colds and infectious pathologies of the upper respiratory tract, that is, the throat and nasopharynx, and require special examination and treatment by an otolaryngologist.
Sinusitis can be acute: catarrhal, purulent, polymeric, as well as chronic. These diseases require special treatment with antibiotics, antivirals and possibly antifungals. This inflammatory process threatens with such serious complications as meningitis, arachnoiditis and encephalitis (this is inflammation of the hard arachnoid membrane of the brain and the substance of the brain).
Science does not stand still, new methods of treating diseases are being created, drugs are being produced that can quickly and easily cure and correct defects. But all prescriptions are made exclusively by the doctor, based on the results of the examination. There is no point in doing something on your own, since in this case it can lead to undesirable consequences. Therapy is carried out only under the supervision of the attending physician and according to his recommendations.
The influence of aplasia on the occurrence of sinusitis
In cases of incomplete recovery or with advanced frontal sinusitis, the disease can take a chronic form. This is dangerous due to frequent relapses of the disease and other serious consequences in the form of meningitis or inflammation of the brain.
There is congenital hypoplasia, acquired or secondary.
A doctor can diagnose a unilateral form of pathology. For example, there is hypoplasia of the frontal sinus on the right. What this is is already clear from the name. Of course, this is not the only scenario. Hypoplasia of the left frontal sinus also occurs with the same frequency. The doctor will tell you what it is if he discovers such an anomaly.
The formation of frontal sinuses is a genetically programmed process. Every child is born without them, that is, a newborn baby does not have them at all. The frontal sinuses normally begin to develop at about 7-8 years of age and by the age of 25 this process ends. Their cavity in an eight-year-old child is a maximum of 0.7 cm3, and in adults it reaches 7 milliliters.
Functions of the frontal sinus or frontal sinus:
- reducing the mass of the skull, making it lighter;
- protection of the brain from injury, a kind of shock absorption;
- acoustic function, formation of a characteristic voice timbre;
- individuality of facial features;
- moisturizing the mucous membranes of the nasal cavity.
Agenesis or atresia of the frontal sinuses can also be acquired. Such hypoplasia is essentially secondary sclerosis. This occurs as a result of past infections - frontal sinusitis, pansinusitis, or injuries to the facial area. Their consequences are regression of cavity development and bone compaction.
This is frontal sinusitis, sinusitis, ethmoiditis or inflammation of the mucous membranes of all sinuses at once (pansinusitis). Such diseases are complications of colds and infectious pathologies of the upper respiratory tract, that is, the throat and nasopharynx, and require special examination and treatment by an otolaryngologist.
Sinusitis can be acute: catarrhal, purulent, polymeric, as well as chronic. These diseases require special treatment with antibiotics, antivirals and possibly antifungals. This inflammatory process threatens with such serious complications as meningitis, arachnoiditis and encephalitis (this is inflammation of the hard arachnoid membrane of the brain and the substance of the brain).
Science does not stand still, new methods of treating diseases are being created, drugs are being produced that can quickly and easily cure and correct defects. But all prescriptions are made exclusively by the doctor, based on the results of the examination. There is no point in doing something on your own, since in this case it can lead to undesirable consequences. Therapy is carried out only under the supervision of the attending physician and according to his recommendations.
Birth defects and anomalies can be directly related to hereditary pathology, when the normal process of formation of other cranial parts is disrupted. For example, abnormal development of the maxillary sinuses (maxillary sinuses) is detected in 13 percent of children diagnosed with sinusitis. Most often, anomalies of the paranasal sinuses manifest themselves as follows:
- A person’s sinuses may be partially narrowed or completely absent as a result of excess pressure on them from the facial or nasal walls. In this case, underdevelopment will vary widely, starting with a slight depression of the canine fossa, and ending with complete fusion of the nasal wall and the facial wall. In the latter case, the sinus simply disappears in the lower section.
- Doctors often diagnose unilateral anomalies. In this case, facial asymmetry is clearly visible. When attempting to puncture (puncture) an underdeveloped sinus, the doctor’s needle passes into the soft tissue of the cheek.
- Anomalies and defects of the frontal sinuses will differ from each other in both their size and volume. In some clinical cases, doctors diagnose agenesis of the frontal sinuses with a volume of up to 500 milliliters. There are four main types of delay in the development of sinuses. We are talking about a violation of pneumatization or its complete absence, unilateral or bilateral aplasia of the frontal sinus, trabecular agenesis and secondary sclerosis (regressive type anomaly).
- It is worth noting that aplasia is most often diagnosed in men. In addition, with unilateral disorders, the most reliable diagnosis is poor development of the opposite sinus.
Structural features
The paranasal sinuses are represented by cavities internally covered with epithelial tissue. Most of them are located in the bones of the facial skull or within the anterior cranial fossa.
The epithelium, which is characteristic of the sinuses, performs an excretory function - microparticles of dust, pollen and other particles deposited on the epithelium are removed. The goblet cells contained in the epithelium perform the function of producing mucus, which, together with the movement of the cilia of the ciliated epithelium, ensures the removal of foreign particles and supports the self-cleaning of the paranasal sinuses.
Another important function is to humidify and warm the air while it is in the sinuses. Also, the sinuses themselves perform a resonator function for the voice - they provide its tonality, sonority and individual coloring. Thus, they are quite important structures of the human body.
The frontal sinuses are located directly in the thickness of the frontal bone posterior to the superciliary arches. They communicate with the nasal cavity through the middle meatus via the frontonasal canal.
A characteristic feature of the frontal sinus is that at birth this sinus is absent - it develops only by the 7-8th year of life, reaching its maximum development by puberty - for boys - 13-14, for girls - 12-13 years.
The video in this article will help you get acquainted with the detailed structure of the paranasal sinuses and will allow even people far from medicine to form a certain idea about their location:
Anatomy of the frontal sinuses and the concept of frontal sinuses
The frontal sinuses are two cavities in the frontal bone of the skull, located to the left and right of the midline. Their size and configuration vary individually among different people. Frontal sinusitis in children, especially small ones, is quite rare, since their frontal sinuses are not yet formed.
The frontal sinus is limited by four walls. The lower wall separates it from the orbit, the back wall is adjacent to the anterior cranial fossa, the middle wall is the wall between the right and left frontal sinuses. The front thick wall is the human forehead. Inside, the frontal sinuses can be relatively “smooth”, or they can be divided by bony projections and septa into many cells.
In the lower wall of the cavity there is a hole leading into a canal connecting the sinus with the middle nasal passage. The downward frontonasal canal should provide free outflow of the contents of the frontal sinus. But it is quite long (from 15 to 25 mm) and narrow (from 1 to 4 mm), so with the slightest swelling of the mucous membrane, the outflow from the sinus sharply worsens. And the lack of drainage is a direct path to the development of the inflammatory process.
Frontal sinusitis is an inflammation of the mucous membrane lining the inside of the paranasal frontal sinuses. Depending on the nature of the disease, it can be acute or chronic.
Classification of sinuses by type of structure
There are also several types of paranasal sinuses according to their type:
- Pneumatic type;
- Sclerotic type.
The frequency of occurrence of frontal sinuses can be affected by the type of sinus - in the presence of a sclerotic type, more favorable conditions are created for the development of the pathological process in it.
This type of sinus is characterized by:
- significant reduction in size;
- the presence of thick bone structures;
- small, limited cavity.
This cavity, when pathogenic microflora enters it, serves as a fairly good reservoir, which ensures the proliferation of microorganisms, and due to its structural features, there is a violation of the evacuation and removal of foreign particles along with mucus.
Hypoplasia
Hypoplasia of the frontal sinuses is an underdevelopment of these formations. This condition can be genetically determined, or develop in the embryonic period under the influence of various factors.
Most often, sinus hypoplasia is detected in adolescence, when the process of final formation of the sinus occurs.
The presence of sinus hypoplasia increases the risk of developing certain diseases:
| Frontit | Inflammation of the mucous membrane of the frontal sinus |
| Mucocele | A protrusion of the mucous membrane, which is a small cyst that can be associated with a bacterial infection |
| Polyposis | Formation of specific outgrowths of the sinus mucosa - polyps |
Most often, the development of the above conditions is the reason for sending a person for research, where hypoplasia is detected. Changes in the sinuses lead to disruption of their functions (insufficient warming, air humidification, maintaining the timbre of the voice) and require treatment by an otolaryngologist.
Concomitant deviated septum is not uncommon. This condition does not affect the incidence of sinus hypoplasia, but is a factor that increases the risk of developing infectious complications.
A deviated septum can be corrected through surgery. This is a necessary measure in case of frequent frontal sinuses or in severe cases of the inflammatory process.
The condition of sinus hypoplasia is not accompanied by characteristic symptoms. Many people who have it do not feel any discomfort. Quite often, hypoplasia is detected by chance on an x-ray, after the development of frontal sinusitis.
Hypoplasia can be detected using additional research methods: radiography, computed tomography.
In the event of frontal sinusitis or other sinus pathologies, it is imperative to contact an ENT doctor - a specialist who treats pathological processes in the sinuses. This specialist will be able to provide qualified assistance and draw up step-by-step instructions for resolving the problem.
It is not possible to cure sinus hypoplasia. ENT doctors treat complications that develop in the altered sinus.
For inflammatory diseases, this is drug treatment. For cysts and tumors, surgical interventions may be prescribed. But, most often, patients with this diagnosis lead a normal life and this structural feature does not bother them in any way.
Mucocele of the frontal sinus
Signs
The disease develops slowly, and the first symptoms do not appear immediately. First, a headache appears, and the pain is mainly in the forehead area. The pain gradually progresses, after a while the area around the eye begins to hurt. Impaired color vision and diplopia (double vision) may occur. The eyeball moves down and out, and a rounded protrusion appears in the corner of the orbit. If you press on the protrusion, a crunching sound is heard. As a result of pressure, a fistula (a canal connecting the cavity of an organ with the environment or the cavity of another organ) can form, through which viscous mucus is released. Possible lacrimation.
Description
Mucoceles can develop in sinuses that have narrow excretory ducts or openings, that is, the frontal sinus, ethmoidal labyrinth, and sphenoid sinus. It occurs when the duct is closed. And it can close due to any developmental pathologies, trauma, tumor, curvature of the nasal septum, formation of scars or adhesions. In addition, fluid is required for mucocele formation. It is produced during inflammation of the mucous membrane. Moreover, if the fluid is purulent, then the disease is called pyocele.
Mucocele and pyocele usually affect school-age children. Several years may pass from the start of a pathological process, for example, a nasal injury, to the appearance of the first symptoms. This usually takes 1-2 years, but there are cases where the disease developed gradually over 15 years. Therefore, adults suffering from this disease often consult a doctor.
The growth of a mucocele can lead to stretching and thinning of the sinus walls, and later to disruption of the integrity of the septum between the sinuses and their walls. In addition, the pathological process can spread to other sinuses and tissues and cause empyema (accumulation of pus inside a cavity). Mucocele can also cause meningitis.
Diagnostics
The diagnosis is made based on examination data and characteristic signs of the disease. You also need to do an x-ray, diaphanoscopy or computed tomography of the frontal sinuses. The latter is more informative.
Sometimes a sinus puncture is performed. At the same time, viscous liquid flows out of the sinus. Its color ranges from transparent light yellow to light brown. Cholesterol crystals are often found in it.
Mucocele of the frontal sinus is differentiated from tumors and dermoid cyst. Unlike oncological diseases, with mucocele the general condition of the patient does not worsen. A dermoid cyst can be distinguished by X-ray results.
Treatment
Mucocele and pyocele are treated only surgically. In this case, the wall of the sinus that presses into the eye socket is removed. Some doctors advise curettage of the sinus mucosa, since the glandular apparatus of the remaining mucosa may work too hard, which will lead to recurrence of the mucocele. However, there is evidence that you don't have to do this.
But it is imperative to expand the anastomosis of the sinuses and nose to improve the outflow of mucus formed.
The prognosis of the disease with timely treatment is favorable.
Prevention
To prevent mucocele, you need to promptly treat inflammatory diseases of the upper respiratory tract, try to prevent nasal injuries, and avoid hypothermia. If you have any suspicious symptoms, you should consult a doctor rather than try to treat yourself.
© Dr. Peter
Aplasia
Interesting, but a little alarming for most, is the fact that in a small number of people - 4-5% - the frontal sinuses are completely undeveloped.
In most cases, people with sinus aplasia lead a full, normal life and this feature does not interfere with them in any way. But, in some cases, specific processes are still possible, the risk of which steadily increases in the presence of hypoplasia or aplasia of the frontal sinus.
Frontal sinus aplasia is a condition in which the frontal sinuses are not fully developed. The formation of the sinuses begins in the prenatal period.
Sinus aplasia can occur under the influence of the following factors:
- Exogenous – environmental factors: unfavorable environment, poor nutrition of the mother, bad habits, etc.;
- Endogenous - factors of the internal environment - taking medications that have a teratogenic effect, genetic predisposition of the mother.
Aplasia can be unilateral or bilateral.
In the case of bilateral aplasia, there will be no risk of developing inflammatory diseases - this condition is characterized by a complete absence of grooves. However, disturbances in air warming and a slight increase in intracranial pressure will be detected, which may affect the well-being of patients with bilateral aplasia.
This condition is diagnosed by an x-ray or computed tomogram, which clearly shows the complete absence of the paranasal sinuses.
There is no reason to worry in the case of unilateral localization of aplasia - the absence of a sinus does not affect the incidence of inflammatory diseases in the sinus.
If you experience discomfort in the forehead area or symptoms of frontal sinusitis, you must consult a doctor. Frequent inflammation of the frontal sinus is a reason to take an X-ray for preventive purposes - it will allow the doctor to exclude or confirm hypo- or aplasia of the frontal sinuses and make a correct diagnosis in case of other causes of inflammation.
Acute form
The structure of the frontal sinuses characterizes the symptoms of the disease. So, with frontal sinusitis, there is a sharp pain in the forehead, which can intensify when pressing on the front wall of the sinus. You can check this by pressing yourself on the area above the bridge of the nose. If the pain intensifies, frontal sinusitis can be assumed. The pathology also causes the following symptoms:
- Pain in the eyes;
- photophobia appears;
- copious discharge appears from the nose;
- sometimes there is a change in the color of the skin above the eye;
- symptoms of general intoxication are observed;
- Body temperature rises to 39.
During the examination, the ENT specialist may detect swelling and hyperemia of the nasal mucosa.
During acute frontal sinusitis, when the outflow of mucus from the sinuses is disrupted, the pain syndrome intensifies. However, as soon as the lumen of the tubule increases and the contents can exit, the pain subsides. Periods of stagnation are usually observed in the morning hours. At this time, pain can radiate to the eyes and temples.
If the acute form of the pathology is not treated, it becomes chronic. This can also happen due to improperly selected treatment.
Clinically, chronic inflammation of the frontal sinus occurs with the following symptoms:
- pressing pain in the frontal cavity, which increases with tapping;
- There is abundant purulent discharge from the nose;
- in the morning there is abundant purulent sputum.
All these symptoms are less pronounced. Because of this, many believe that the disease has receded. In fact, it went from acute to chronic. If left untreated, the disease can cause serious complications.
Frontal sinuses
The frontal sinuses are paranasal sinuses located in the frontal bone behind the brow ridges. Their lower walls are represented by the anterior walls of the orbits, the posterior walls protect the sinuses from the frontal lobes of the brain. The inside of the cavities is lined with mucous membranes. It is worth noting that such cavities are absent in young children; they begin to develop only by the age of 8, completing their formation by 18-21 years. The height of the frontal sinuses in an adult reaches 30 mm, width 25 mm, depth 20-25 mm, volume does not exceed 8 ml.
The absence of frontal sinuses is not a pathology; it is diagnosed in 5% of the population. The frontal sinuses are necessary to ensure the normal functioning of the body. Due to the fact that these cavities are absent in newborns and young children, doctors conclude that one of the main functions of such formations is to reduce the mass of the skull. In addition, the sinuses provide:
- protecting the brain from shock;
- in the cavities, the air comes into contact with the mucous membranes, while being moistened and warmed;
- participate in the process of formation of the human voice, enhance the response.
The frontal sinuses are not developed - what does this mean?
It is known that at birth in newborns the frontal recess is not fully developed or is completely absent. The accessory cavities begin their formation while in the mother's belly , but complete their formation only closer to the age of 18 or during puberty.
If, upon examination by a doctor, it was diagnosed that the child’s frontal sinus is not developed, there is no need to be afraid.
The largest region, called the maxillary region, is formed only at adulthood , and before that time each section of the frontal sinus can be pneumatized.
If there is a suspicion of undeveloped frontal sinuses in an adult, the doctor may send for additional examinations. This is necessary if there is a risk of disease formation due to the penetration of viruses or microbes, as well as if there is a risk of a tumor or cyst.
It is known that with reduced pneumatization, disease of the maxillary region occurs. This most often occurs when the area of the lower septum is too elastic. In addition, if the right frontal sinus or both parts at once are undeveloped, the patient often complains of pain in the head and temporal region, as well as a feeling of constant pressure on the bridge of the nose.
A common cause of frontal disease is the anatomical structure. When examined on an x-ray at this time, it is clear that the paranasal cavities are filled with air. In this case, the patient is given treatment in which the general condition is normalized and excess air flows are removed. With poor quality or incorrect therapy, disease in this area leads to consequences that are dangerous for overall health.
It is important to note that children do not have frontal sinuses at all. Before the age of eighteen, they are just beginning to develop and form in the upper part of the eyes. Towards the completion of formation, this side grows into the mucous region of the nose and becomes covered with mucous membrane.
At the same time, dissolution of the spongy bone occurs , which is located between the inner bone and the outer part of the skull.
Features of the structure of the frontal sinus
The frontal sinus is located in the frontal bone behind the brow ridges. The cavities are presented in the form of paired formations, shaped like a pyramid with three sides. The septum of the frontal sinuses separates the right and left sinuses. In most cases, they are asymmetrical, this is due to the fact that the bony septum is tilted in one direction. Their inner surface is lined with mucous membranes.
The cavities consist of the following walls:
The base of the sinus is the upper wall of the orbit. The anterior wall of the sinus is the densest, it can be felt, it is located 1-2 cm above the eyebrows. The back and bottom walls are aligned at right angles. It is worth remembering that deviations in the structure of the frontal sinuses are not uncommon; for example, in some patients the internal septum is not located vertically, but horizontally. The cavities in this case are located one above the other.
Frontal sinus aplasia
Aplasia is the absence of an organ or its presence in a rudimentary, underdeveloped state. So it cannot function fully, which can sometimes become a predisposing factor for certain diseases.
Aplasia of the frontal sinuses occurs no more often than in 3-5% of patients in the ENT department. Some doctors replace this term with agenesis, atresia or hypoplasia, since these definitions are synonymous.
The structure of the frontal sinuses
The frontal sinuses are a continuation of the paranasal sinuses, that is, the paranasal sinuses. They are located immediately under the brow ridges, being the upper walls of the eye sockets. The average size ranges from 2-3 cm, and the volume can reach 7 ml. The production of mucus in the organ is controlled by the supraorbital nerve.
In newborns, the frontal sinuses are completely absent. The main formation of the organ ends by the age of 8 years. The maximum size of the cavity is reached only when a person is 25 years old.
Often these sinuses are asymmetrical in size, and the septum between them can be deviated to the right or left. Hypoplasia of the frontal sinuses is the complete absence of one or two sub-brow cavities.
Causes of aplasia
Aplasia of the frontal sinus is a congenital defect directly related to a malfunction in the genetic code of the fetus or exposure to teratogenic factors on a pregnant woman.
These include the following impacts:
- chemical;
- biological;
- mechanical.
That is, any incorrect actions of the mother during pregnancy can affect the full development of the unborn child. For example, taking any strong medications, abdominal injuries, smoking, drinking alcohol, poor lifestyle or dangerous work.
Sometimes aplasia is inherent in the patient's genetic code. Therefore, if such an anomaly was found among relatives of even the most distant generations, we can confidently speak about a hereditary predisposition.
Signs of anomaly
Hypoplasia of the frontal sinus is an anomaly that is rarely diagnosed in completely healthy patients. Most often it is detected when a person goes to the doctor with any complaints. There are several signs that distinguish aplasia.
These include the following features:
- Sometimes narrowing of the paranasal sinuses develops due to pressure on them from the facial or nasal wall. In some patients this anomaly will involve depression of the canine fossa, in others it will involve fusion of the nasal and facial walls.
- If a person is diagnosed with unilateral underdevelopment of the frontal sinuses, asymmetry on the face is observed with the naked eye.
- Sometimes the presence of an underdeveloped sinus is revealed during puncture. When performing a puncture, the specialist notes that the needle passes through the soft tissue of the cheek.
- If the anomaly is one-sided, in the absence of one sinus, the second will also be underdeveloped.
- Most often, aplasia is diagnosed in males.
- Sometimes the inflammatory process in the body provokes regression in the development of existing sinuses. In this case, the cavities can significantly decrease in size.
However, the presence of any signs or predisposing factors in the patient’s life does not guarantee the occurrence of pathology in the structure of the sinuses. You can find out for sure about their presence or absence only after a high-quality diagnosis.
How is it diagnosed?
There are several types of diagnostics that help determine the presence of any pathological processes in the frontal sinuses. To conduct a full examination using equipment, you need to consult an otolaryngologist.
For diagnosis the following is carried out:
- X-ray examination. X-ray helps determine the enlargement of the sinus, the structure of the septum in this organ, and the severity of its contours.
- Computed tomography (CT). It is the same scan using an X-ray machine, but with CT, the organ is studied using layer-by-layer sections. This helps to more accurately determine the location of the cavity, its structure and the thickness of the bone wall between the sinuses. Computed tomography also helps to identify inflammatory processes, degenerative changes in the facial bones and other anomalies.
- Ultrasound examination (ultrasound). Non-invasive and safe diagnostic method. It is often used in young children due to the absence of any pain, as well as harmful effects. It is often prescribed when the doctor has doubts about the data obtained after an x-ray.
- Magnetic resonance imaging (MRI). It is one of the most highly informative diagnostic methods. The resulting image has high contrast, helping to identify the presence of a tumor or inflammatory process in the area. A significant advantage of MRI is the absence of x-ray radiation with a high quality diagnostic examination.
As a rule, hypoplasia is diagnosed using these techniques when a patient presents with any complaints. That is, the anomaly is rarely detected on its own. Most often, a person learns about it when any disease appears in this area.
Diseases of the frontal sinuses
It is worth remembering that the frontal sinuses are hollow formations, the surface of which is lined with mucous membranes. Such formations are quite often affected by bacteria and viruses. Representatives of pathogenic microorganisms enter the human body with inhaled air, and if the human immune system fails, the following diseases occur:
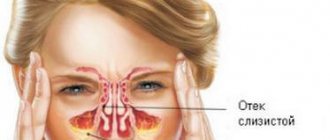
With frontal sinuses, inflammation forms on the mucous membranes, after which it penetrates through the nasolacrimal duct to the frontal sinuses. As a result, swelling occurs, the excretory canal is blocked, and as a result, the outflow of mucous contents from the sinus is limited or blocked. It should be remembered that the treatment of such a disease must be comprehensive; it is impossible to cure frontal sinusitis without antibiotics.
The cyst is a small round container with thin walls. It can have different sizes. The causes of cysts are similar to the prerequisites for the occurrence of frontal sinusitis. During the inflammatory process, fluid is constantly produced (possibly in an increased volume), but its outflow does not occur. Consequently, due to the accumulation of mucus, a cyst is formed. In this case, drug treatment is ineffective; surgery is indicated.
Functions of the frontal sinuses
Along with other paranasal cavities, the frontal sinuses serve for the efficient functioning of the body. Given the fact that they are absent at birth, there is a hypothesis that the main function of the frontal sinuses is to reduce the mass of the skull. In addition, the frontal cavities:
- act as a kind of shockproof “buffer” that protects the brain from injury;
- participate in the breathing process: air from the nasal passages enters the cavities, where, interacting with the mucous membrane, it is additionally moistened and warmed;
- take part in the formation of sounds and increase vocal resonance.
Causes of inflammation
The bones of the skull, which have a porous structure, are lined with mucous membranes in order to provide the body’s protective function, which is to prevent the penetration of various particles and microorganisms that can become a source of pathology. But it is worth remembering that with a decrease in immunity, pathogenic microorganisms can easily penetrate the human body .
Due to the fact that the frontal sinuses are connected to the nasopharynx, when severe pathology develops, pathogens penetrate them and cause the development of polysinusitis - inflammation of all paranasal sinuses, including the frontal ones. The development of infection can be triggered by hypothermia, poor nose-blowing technique, lack of proper treatment of the underlying disease, interruption of antibacterial therapy, and non-compliance with the treatment regimen.
Infection
In more than half of cases of frontal sinusitis, the frontal sinuses become inflamed due to infection that enters the cavity through the tubules. The inflammatory process can occur in several sinuses at once, for example, the maxillary sinus and frontal sinus can be affected. The cause of inflammation can be ARVI, diphtheria, tonsillitis and other infections.
The most common causative agents of inflammation are:
- rhinoviruses;
- adenoviruses;
- coronaviruses;
- different types of bacteria;
- fungi.
Therapy technique
Drug treatment of sinusitis does not differ from the treatment of inflammation of the paranasal sinuses, therefore it is carried out in the same directions:
- The use of antibacterial drugs macrolides, cephalosporins, penicillins.
- Use of anti-inflammatory drugs.
- Taking antiallergic medications to relieve swelling.
- Steam inhalations.
- Irrigation of the nasal cavity with saline solution.
- The use of nasal drops and sprays of various effects.
- Physiotherapy.
- Breathing exercises by Strelnikova.
- Use of immunostimulating drugs.
It should be remembered that only a doctor should prescribe treatment. Self-medication is unacceptable; it can lead to a number of irreversible consequences.
Consequences and complications
Possible complications of inflammation of the frontal sinus include:
- Difficulty breathing, which leads to chronic hypoxia. This condition negatively affects the condition of all organs and systems of the body. It is worth remembering that this complication is especially dangerous for children - it can cause developmental delays.
- Breathing disorder during sleep. Against this background, constant drowsiness occurs.
- The development of blindness is possible. Against the background of chronic inflammation, photophobia and decreased visual acuity develop.
- Development of inflammatory processes in ENT organs.
- Meningitis.
- Encephalitis.
- Brain abscess.
At the very beginning of the inflammatory process, it is extremely important to consult a doctor and unquestioningly follow all his recommendations and instructions. It is worth remembering that only correct and timely treatment will overcome the pathology and cope with the symptoms of inflammation. Without treatment, the consequences can be irreversible.
Chronic form
The structure of the frontal sinuses characterizes the symptoms of the disease. So, with frontal sinusitis, there is a sharp pain in the forehead, which can intensify when pressing on the front wall of the sinus. You can check this by pressing yourself on the area above the bridge of the nose. If the pain intensifies, frontal sinusitis can be assumed. The pathology also causes the following symptoms:
- Pain in the eyes;
- photophobia appears;
- copious discharge appears from the nose;
- sometimes there is a change in the color of the skin above the eye;
- symptoms of general intoxication are observed;
- Body temperature rises to 39.
During the examination, the ENT specialist may detect swelling and hyperemia of the nasal mucosa.
During acute frontal sinusitis, when the outflow of mucus from the sinuses is disrupted, the pain syndrome intensifies. However, as soon as the lumen of the tubule increases and the contents can exit, the pain subsides. Periods of stagnation are usually observed in the morning hours. At this time, pain can radiate to the eyes and temples.
If the acute form of the pathology is not treated, it becomes chronic. This can also happen due to improperly selected treatment.
Clinically, chronic inflammation of the frontal sinus occurs with the following symptoms:
- pressing pain in the frontal cavity, which increases with tapping;
- There is abundant purulent discharge from the nose;
- in the morning there is abundant purulent sputum.
All these symptoms are less pronounced. Because of this, many believe that the disease has receded. In fact, it went from acute to chronic. If left untreated, the disease can cause serious complications.