What is cholesteatoma?
Cholesteatoma is a capsule with a cavity inside. This cavity contains desquamated epithelial cells, as well as cholesterol in the form of crystals. The size of this neoplasm varies from a few millimeters to seven centimeters. Experts do not classify cholesteatoma as a tumor-like formation, since its structure is complex and multilayered.
- The capsule is a kind of barrier to neoplasm, consisting of connective tissue. The inner part of the capsule is covered with keratinizing squamous epithelium;
- The middle layer consists of deflated epithelium, which is arranged in a kind of layers, between which there are cholesterol crystals;
- In the center of the cholesteatoma there is a core, which consists of whitish debris (adipose tissue). Detritus has a specific putrefactive odor.
Cholesteatoma can form as a single formation or in the form of many nodules representing a dense formation. Cholesteatoma releases toxic compounds, which subsequently worsen the quality of hearing perception, and also lead to the occurrence of inflammatory processes in the labyrinth of the ear. These chemical elements are capable of melting bone structures and spreading into the cranial cavity, into its middle and posterior cranial fossae.
Leading clinics in Israel
Assuta
Israel, Tel Aviv
Ikhilov
Israel, Tel Aviv
Hadassah
Israel, Jerusalem
Causes of the disease
In medical practice, there are two types of cholesteatoma:
- Congenital . It has a second name: “true”. Education begins in the intrauterine development of the fetus. Its structure is smooth, which is why it is called a pearl tumor. Most often it forms in the pyramid of the temporal bone.
- An acquired type of cholesteatoma, also called false, can form with age. The reason for their formation may be advanced otitis media, trauma to the ear for one reason or another, for example, submariners often suffer from occupational trauma, the so-called barotrauma. Factors that provoke the development of cholesteatoma with age are the following:
- A person is diagnosed with eustachitis - when the patency of the auditory tube is disrupted due to inflammatory processes in the eustachian tube. A large tympanic cavity is formed due to the fact that the pressure in the tympanic cavity decreases. As a result, the eardrum is retracted into it and cholesterol crystals and desquamated epithelial cells collect inside this cavity;
- Part of the eardrum is injured . The cause may be otitis media or trauma. In the resulting area of the ear, the flat epithelium begins to grow into the tympanic cavity. Cholesteatoma is formed. According to statistics, the cause of acquired cholesteatoma in 90% of cases is the chronic form of purulent otitis.
Congenital cholesteatoma of the middle ear
DescriptionCase ICase IICase III
Description
Congenital cholesteatomas are rare but increasingly diagnosed tumors in children that develop from surviving embryonic cells. The main diagnostic criterion is the presence of a tumor behind a preserved and previously undamaged eardrum. Congenital cholesteatomas grow slowly, and the course of the disease is often asymptomatic. As they grow, they cause damage to the eardrum, auditory ossicles and temporal bone. When perforation of the tympanic membrane occurs, it is impossible to distinguish congenital cholesteatoma from acquired one. Symptoms correlate with the degree of destruction of individual structures of the middle ear and temporal bone, and most often include hearing loss. Without treatment, they can cause complications that can threaten the health and life of the child. These include: paresis and paralysis of the facial nerve, dizziness with loss of labyrinthine function, meningitis, abscesses of the temporal lobe and cerebellum. These complications develop even in our era of widespread use of antibiotics. Congenital cholesteatomas are sporadically diagnosed even in adult patients. It should be noted that in comparison with adult patients, in children the course of the disease is more aggressive and more often causes serious complications.
Case I
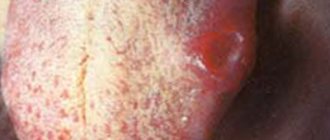
The photograph shows congenital cholesteatoma of the middle ear. A whitish mass fills the middle ear. Right ear, 5 year old child. Cholesteatoma is located in front of the manubrium of the malleus in the anterior and superior quadrants, that is, in the typical location most often described in the literature. Other regular anatomical structures are visible, including the manubrium of the malleus. Cholesteatoma in such a place does not make itself felt for a long time, the course is asymptomatic. Does not lead to destruction of the auditory ossicles, which are located in the posterior quadrants. It can cause hearing loss and exudative otitis media if it grows towards the mouth of the auditory tube. Exudative otitis media may mask the presence of a tumor in the middle ear. It must be remembered that chronic inflammation that cannot be treated should persuade the doctor to refer the child to a specialist.
In this case, cholesteatoma was asymptomatic and the diagnosis was made during routine examination. It is difficult to diagnose congenital cholesteatoma in such a location, especially in young children, when the anterior quadrants of the eardrum are poorly visible.
Congenital cholesteatoma of the middle ear
Congenital cholesteatoma of the middle ear - diagram
- short process of the malleus
- hammer handle
- navel eardrum
- congenital cholesteatoma in the anterior and superior quadrants
- Treatment of congenital cholesteatoma is exclusively surgical. If you suspect this disease, it is necessary to refer the child to a specialized center where operations are performed on children.
- In this case, the operation was performed only through the external auditory canal.
- The cholesteatoma was removed entirely in the form of an oval tumor with a diameter of 0.5 cm.
- There was no need for reconstruction of the eardrum and ossicles.
- The prognosis is favorable with early diagnosis.
- There is usually no need for second-look revision surgery, since possible regrowth of the cholesteatoma can be seen on video-otoscopic examination.
Case II
The photograph shows congenital cholesteatoma of the middle ear. A whitish mass fills the middle ear. Left ear, 6-year-old child. Two air bubbles and an amber exudative effusion are visible below and in front. Other anatomical structures, including the manubrium of the malleus, are not visible. Cholesteatoma in this position has already partially destroyed the auditory ossicles and is growing posteriorly towards the mastoid cavity. Diagnosing congenital cholesteatoma using an otoscope in this position is not difficult.
Symptoms include intermittent ear pain, sensations of throbbing and fullness in the ear, and marked hearing loss as a result of the presence of effusion and swelling in the ear and destruction of the auditory ossicles. Quite often, congenital cholesteatomas are the cause of exudative otitis media if they grow towards the mouth of the auditory tube, causing its obstruction, as can be seen in the photograph. Exudative otitis media may mask the presence of a tumor in the middle ear.
Congenital cholesteatoma
- Treatment of congenital cholesteatoma is exclusively surgical. If you suspect this disease, it is necessary to refer the child to a specialized center where operations are performed on children.
- In this case, the operation was performed through access through the external auditory canal, as well as through anthromastoidectomy and posterior tympanotomy, i.e. access to the middle ear through the facial recess (recessus facialis).
- The tympanic membrane is strengthened using a flap from the fascia of the temporalis muscle.
- At the same time, reconstruction of the auditory ossicles was performed using a titanium TORP prosthesis.
- Ossiculoplasty was performed using an artificial prosthesis, since cholesteatoma destroyed both the incus and the superstructure of the stapes.
- As a rule, a repeat revision operation is required, the so-called. “second-look” operation, 6 months after the first.
- Surgery for cholesteatoma in children is much more difficult than in adult patients, this is due to the fact that the child’s temporal bone contains thousands of small cells and depressions where epithelium and cholesteatoma can accumulate.
Case III
The photograph shows congenital cholesteatoma of the middle ear. Right ear, 8 year old child. A whitish mass completely fills the middle ear cavity. The anatomical structures of the middle ear are not visible, and the eardrum is significantly bulging due to the presence of cholesteoma. Cholesteatoma in this position has already partially destroyed the auditory ossicles and grows posteriorly towards the cavity of the mastoid process and fills all the recesses of the tympanic cavity and the mastoid process.
Diagnosing congenital cholesteatoma using an otoscope in this position is not difficult. It is necessary to differentiate from the late stage of tympanosclerosis, although this disease practically does not occur in young children without a history of otitis media. \n\nSymptoms most often include hearing loss, as a result of the presence of a tumor in the ear and destruction of the auditory ossicles, as well as periodic pain and a feeling of ear fullness. For a long time, choleosteatoma may not be diagnosed, as it grows slowly and the child gradually gets used to the symptoms of the disease.
Congenital cholesteatoma
- Treatment of congenital cholesteatoma is exclusively surgical. If you suspect this disease, it is necessary to refer the child to a specialized center where operations are performed on children.
- In this case, the operation was performed through access through the external auditory canal, as well as through anthromastoidectomy and posterior tympanotomy, i.e. access to the middle ear through the facial recess (recessus facialis).
- A part of the eardrum was removed, since the cholesteatoma was tightly adjacent to its inner surface and it was impossible to separate it. The tympanic membrane was reconstructed using a flap from the temporalis muscle fascia.
- At the same time, reconstruction of the auditory ossicles was performed using a titanium TORP prosthesis.
- Ossiculoplasty was performed using an artificial prosthesis, since cholesteatoma destroyed both the incus and the superstructure of the stapes.
- As a rule, a repeat revision operation is required, the so-called. “second-look” operation, 6 months after the first.
- Surgery for cholesteatoma in children is much more difficult than in adult patients, this is due to the fact that the child’s temporal bone contains thousands of small cells and depressions where epithelium and cholesteatoma can accumulate.
Signs of illness
Like many diseases associated with neoplasms, cholesteatoma does not make itself felt for a long time. Symptoms indicating hearing impairment associated with cholesteatoma are as follows:
- Feeling of fullness inside the ear;
- Pain in the ear, and only in one;
- A person may suffer from migraines;
- A slight discharge from the ear that has a foul odor;
- The quality of sound perception may deteriorate. There may be several reasons for this. It all depends on the course of the disease. Due to the deterioration of the mobility of the auditory ossicles, the passage of sound waves deteriorates. Another cause of hearing impairment may be that discharge from cholesteatoma damages the receptors of the labyrinth;
- If the formation of cholesteatoma is associated with existing chronic otitis, the person’s temperature rises, weakness occurs, and appetite worsens. The cause of these conditions may be an associated secondary infection, which leads to intoxication of the body.
Symptoms
The patients' complaints are similar to those with chronic otitis - constant or frequent discharge of pus from the ear, decreased hearing (most often the hearing thresholds increase significantly). The discharge often has an unpleasant putrid odor. Hearing loss is of a mixed nature, i.e. There is both a conductive component (due to the destruction of the sound-conducting system of the auditory ossicles and eardrum) and a neurosensory component (due to damage to the sound-receiving hair cells of the inner ear by toxins and inflammatory mediators that are released during chronic inflammation). Pain in the ear is uncharacteristic; its occurrence should alert you to the possibility of intracranial complications. There may be dizziness, signs of facial nerve paresis - facial asymmetry. All of these are indications for emergency hospitalization of the patient.
Complications
Complications of cholesteatoma are inevitable if you do not consult a specialist in a timely manner. These are:
- Although cholesteatoma is not classified as cancer, it has strong destructive effects. This formation is capable of melting bone structures located near it. Reaches the mastoid process and fills the cells. Then it deforms the channels of the labyrinth capsule. In this case, a labyrinthine fistula occurs. The presence of such is indicated by such signs as deterioration of hearing up to complete loss, tinnitus, nausea and vomiting, dizziness;
- When the bone structure of the mastoid process is destroyed, the tumor emerges under the skin of the mastoid region;
- Cholesteatoma can lead to facial nerve paresis. The reason for this is the ability of the formation to melt the facial nerve canal;
- When the walls of the sigmoid sinus are destroyed, thrombosis of this part of the ear occurs;
- The most severe complication of cholesteatoma is aseptic meningitis. The reason for this is the breakthrough of fluid inside the tumor and its spread to the brain;
- Meningoencephalitis - this condition occurs when toxic fluid enters the brain;
- Brain swelling, coma, bacterial infections that lead to irreversible consequences such as meningitis, brain abscess.
Cell division, characteristic of cancer, is not characteristic of cholesteatoma. Such terrible consequences of cholesteatoma are associated with the localization of the tumor.
Its close location to the brain and its release of toxic substances lead to an aggressive effect on areas of the head.
How to recognize the disease and symptoms?
The middle ear is bounded on almost all sides by the bones of the skull. The growth of the tumor is accompanied by compression and destruction of the surrounding structures. Signs of cholesteatoma:
- ear pain or discomfort;
- ear itching;
- watery or foul-smelling purulent ear discharge.
Other clinical manifestations of acquired cholesteatoma of the ear are different and depend on the location of the formation. It could be:
- dizziness;
- temporary hearing loss, even loss;
- tinnitus;
- lack of mobility of part of the facial muscles (facial nerve paresis).
Complaints with cholesteatoma are usually one-sided.
Congenital cholesteatoma of the middle ear is particularly difficult to diagnose. Unlike secondary formations, its development is not accompanied by damage to the tympanic septum. Therefore, during the examination, the otolaryngologist does not find anything unusual.
The disease is asymptomatic for some time. However, as the cyst grows, it begins to block the lumen of the Eustachian tube, stimulating the appearance of exudate in the middle ear cavity. Progression leads to hearing loss on one (with unilateral lesions) or two (with extremely rare bilateral) sides. Typically, the appearance of parental complaints followed by instrumental examination leads to the identification of the cause of deafness.
Diagnostics
If you experience any discomfort in the ear area, you should consult a doctor, since any of the most harmless ear diseases can lead to disastrous consequences, including cholesteatoma.
- The first step in diagnosing the disease is a visual examination of the external auditory canal. This primary type of examination using special instruments is called otoscopy. Damage to the eardrum is detected, as well as the presence of substances with a cheesy consistency in the middle ear;
- Probing of the middle ear cavity. It is used to assess the condition of bone tissue adjacent to the tumor. Also, the probe that is used in this research method makes it possible to clean the middle ear cavity. Experts examine the contents of substances seized using a probe. The presence of cholesterol crystals and exfoliated epithelium confirms the diagnosis of cholesteatoma;
- X-rays are very often used to diagnose the disease, since X-rays can be used to determine the location and size of the tumor;
- Computed tomography is a more advanced type of diagnosis than x-rays, as it makes it possible to examine the formation layer by layer using a three-dimensional image;
- Magnetic resonance imaging is increasingly used in the diagnosis of various diseases, especially in congenital cholesteatoma. A strong magnetic field, as well as the injected contrast agent, provide a complete picture of the tumor;
- To determine the condition of a particular part of the hearing organ, the degree of damage, additional diagnostic methods are used, such as audiometry (for the presence of hearing impairment), tympanometry (the condition of the eardrum), vestibulometry, electronystagmography, stabilography (the condition of the vestibular apparatus).
Prognosis and prevention
Since this neoplasm is not oncological in nature, recovery almost always occurs.
Doctors recommend the following as preventive measures:
- Completely cure rhinitis, otitis media.
- Prevent the emergence of a chronic focus of infection, especially with frequent relapses of ENT diseases.
- Pain in the head is a reason to consult a doctor for a detailed examination.
- Dress for the weather.
- If a tumor is detected in a child, do not refuse surgery, even if the child feels well.
- After surgery, patients should undergo systematic examinations and follow the doctor’s recommendations.
We recommend reading: What are nevi and what do they look like?
It is important to remember that a disease is easier to prevent than to treat. If the development of pathology cannot be avoided, you should urgently seek medical help.
Treatment
There are several methods of therapy, which are determined exclusively by an ENT doctor together with neurologists and other specialists, in the presence of concomitant diseases.
- Conservative therapy . Typically, this type of treatment is used only when the formation is detected in the early stages of development and its localization is not deep, easily accessible to the doctor. Experts prescribe rinsing the ear with special solutions, usually once a day. If this treatment gives results, the patient is recommended to visit an ENT doctor according to the schedule prescribed by him to prevent the recurrence of the tumor;
- Surgery is a frequently used treatment method for this tumor. Surgery to remove cholesteatoma is performed under general anesthesia. How the operation will be performed depends on the stage of the disease, the degree of its destructive effects on surrounding organs, as well as the location. Under the best circumstances, only the cholesteatoma and all its contents are removed. If the neoplasm has made pathological changes to the surrounding tissues, doctors have to perform manipulations to restore some organs, such as the eardrum (myringoplasty), the auditory ossicle (tympanoplasty), and the labyrinth (labyrintomy).
After surgery, the patient remains under the supervision of specialists for several more days. Some time after the operation, the otolaryngologist checks the degree of restoration of the functions of the hearing organ, then makes recommendations on preventive measures in order to avoid complications or the recurrence of cholesteatoma.
Surgery to remove cholesteatoma of the ear
If traditional therapy does not bring the desired effect, the cholesteatoma formation is treated surgically, usually with a mastoidectomy. In this operation, cholesteatoma tissue is removed from the ear by cutting the membrane separating the middle and outer ear.
If the tumor spreads to the auditory ossicles or nearby areas of bone, they are also partially removed. To preserve the patient's hearing, tympanoplasty is performed at the end of the mastoidectomy (restoration of the eardrum and auditory ossicles).
Another method of surgical treatment of cholesteatoma formation is endoscopy. The operation is performed using a surgical microscope and special endoscopic instruments. Such an intervention is classified as minimally invasive methods, since it is carried out through minor punctures.
Minimally invasive operations eliminate the possibility of damage to the meninges and facial nerve and shorten the rehabilitation period. In addition, after endoscopy there are no cosmetic defects left.
Preventive measures
The formation of cholesteatoma can be avoided by following the following recommendations:
- Harden, harden children from early childhood;
- Do not ignore even a common runny nose, especially in children, since untreated colds sometimes lead to irreversible consequences;
- If the presence of a bacterial infection is confirmed, do not neglect antibiotics during treatment.
Any changes in the ear area should alert a person and be a reason to immediately consult a doctor.
Reasons for the development of cholesteatoma of the ear
Cholesteatoma of the middle ear, like other types of similar formations, is sometimes caused by embryonic disorders.
Acquired formations develop for several reasons:
- Long-term otitis media;
- Pathological processes affecting the auditory tube;
- Obstruction or narrowing of the ear canal;
- Mechanical injuries to the membrane separating the middle and outer ears.
To understand what acquired cholesteatoma is will help to determine the main mechanisms of its occurrence, these are:
- Negative changes in the area of the auditory canal due to inflammation of the mucous membrane of the auditory tube;
- Proliferation of the epithelium of the external valve, which equalizes pressure, into the area of the middle ear.
Reviews
Alexandra. My son was diagnosed with cholesteatoma at the age of 3. For a long time we were given different diagnoses and treated for otitis media. When some kind of fluid began to come out of the ear, they did a computed tomography scan. Extensive cholesteatoma was diagnosed. By the time the disease was discovered, the formation had managed to destroy the bones of the middle ear. The operation took eight hours. Despite all precautions, my son relapsed. Now we are waiting for another operation.
Inna. For those who are afraid of the operation to remove cholesteatoma, especially the fact that such an operation is performed under general anesthesia. I want to say that there is nothing wrong with this. I had to undergo this operation twice. Now I even manage without a hearing aid.
Anonymously. Four years ago I had an operation to remove cholesteatoma, but as it turned out later, the operation was unsuccessful. There was more and more discharge with a purulent odor from the ear. I'm practically deaf in this ear. I have another operation ahead of me. I am very afraid, but doctors say that if the operation is not performed in time, cholesteatoma can reach the brain.