Chronic obstructive pulmonary disease is a pathology that has begun to rapidly gain momentum in recent years, and which often causes death in patients over 45 years of age. In this case, the pathological process mainly affects people who smoke.
The disease is insidious in that its first signs, in particular in smokers, appear only 20 years after the start of smoking. For many years, the pathological process can be completely asymptomatic. However, if left untreated, airway obstruction is prone to progression, which entails early loss of ability to work and a reduction in the patient's life expectancy.
That is why the problem of COPD is especially relevant in our time.
Risk group
The diagnosis of COPD in adult men in Russia is observed in every third person who has crossed the threshold of 70 years. Statistics allow us to confidently say that this is directly related to tobacco smoking. There is also a clear connection with lifestyle, namely the place of work: the likelihood of developing pathology is higher when a person works in hazardous conditions and with a lot of dust. Living in industrial cities has an effect: here the percentage of cases is higher than in places with a clean environment.
COPD develops more often in older people, but if you have a genetic predisposition, you can get sick at a young age. This is due to the specifics of the body’s generation of connective pulmonary tissue. There are also medical studies that suggest a connection between the disease and the child’s prematurity, since in this case there is not enough surfactant in the body, which is why organ tissues cannot expand correctly at birth.
What do scientists say?
COPD, the causes of the disease, treatment methods - all this has long attracted the attention of doctors. In order to have sufficient materials for research, data was collected, during which cases of the disease were studied in residents of rural areas and urban residents. The information was collected by Russian doctors.
It was possible to reveal that if we are talking about those who live in a village, then here with COPD the severe course often becomes ineffective, and in general the pathology torments the person much more severely. Endobronchitis with purulent discharge or tissue atrophy was often observed in villagers. Complications with other somatic diseases occur.
It has been suggested that the main reason is the low quality of medical care in rural areas. In addition, in villages it is impossible to do spirometry, which is necessary for smoking men aged 40 years or more.
How many people know COPD - what is it? How is it treated? What happens when this happens? Largely due to ignorance, lack of awareness, and fear of death, patients become depressed. This is equally characteristic of both urban and rural residents. Depression is additionally associated with hypoxia, which affects the patient’s nervous system.
More about the reasons
Effective prevention of COPD is still under development, but people who want to maintain their health should understand how certain causes affect the human body, provoking this pathology. By recognizing their danger and eliminating harmful factors, you can reduce the likelihood of developing the disease.
The first thing that deserves mention in connection with COPD is, of course, smoking. Both active and passive influences are equally negative. Now medicine says with confidence that smoking is the most important factor in the development of pathology. The disease is provoked by both nicotine and other components contained in tobacco smoke.
In many ways, the mechanism of the appearance of the disease when smoking is associated with the one that provokes pathology when working in harmful conditions, since here a person also breathes air filled with microscopic particles. When working in dusty conditions, in alkali and steam, constantly breathing chemical particles, it is impossible to keep your lungs healthy. Statistics show that COPD is more often diagnosed in miners and people working with metal: grinders, polishers, metallurgists. Welders and employees of pulp factories and agricultural workers are also susceptible to this disease. All these working conditions are associated with aggressive dust factors.
An additional risk is associated with insufficient medical care: some do not have qualified doctors nearby, others try to avoid regular medical examinations.
Symptoms
COPD disease - what is it? How is it treated? How can you suspect him in yourself? This abbreviation (as well as its decoding - chronic obstructive pulmonary disease) still means nothing to many. Despite the widespread prevalence of pathology, people do not even know the risk to their lives. What to look for if you suspect pulmonary disease and suspect that it may be COPD? Remember that the following symptoms are typical at first:
If COPD is exacerbating, it is usually due to an infection, which affects:
- shortness of breath (increases);
- sputum (becomes purulent and is released in larger volumes).
As the disease develops, if chronic obstructive pulmonary disease has been diagnosed, the symptoms are as follows:
- heart failure;
- heartache;
- fingers and lips become bluish;
- bones ache;
- muscles weaken;
- fingers thicken;
- nails change shape and become convex.
Causes of COPD
The dominant number of patients suffering from this pathology are heavy smokers, and the ratio of the number of cigarettes smoked and the period during which the patient has had this bad habit is always taken into account. In addition, people who have a weak bronchopulmonary system, even without obvious clinical manifestations of bronchial asthma, are susceptible to the disease.
In addition, people who are susceptible to COPD are:
- with low body weight;
- those suffering from frequent relapses of respiratory diseases (especially children);
- are passive smokers;
- exposed to unfavorable environmental conditions for a long period of time.
Chronic obstructive pulmonary disease can also develop in non-smoking patients. In this case, we are talking about a person’s genetic predisposition to this pathology. A lack of alpha-trypsin leads to an imbalance between the ratios of protease and antiprotease activity of lung tissue.
Normally, the impact of protease activity in the form of neutrophil elastase, tissue metalloproteinase, destruction of connective tissue structures and elastin occurs. This promotes the regeneration of lung parenchyma.
As for the antiprotease activity of alpha-antitrypsin and secretory proteinase inhibitor, its main task is to regulate the processes of elastin destruction. It is in this regard that patients with COPD constantly exhibit manifestations of antiprotease activity. In this regard, destructive changes in lung tissue occur. Activation of neutrophils causes the development of bronchospasm, excessive production of intrabronchial mucus and severe swelling of the mucous membranes of the respiratory tract.
Severe COPD is always accompanied by a secondary infection, which occurs against the background of decreased mucus clearance in the projection of the distal respiratory tract. Repeated infection of the bronchi causes exacerbation of COPD, which leads to a significant worsening of the underlying pathology.
Thus, the disease has its own pathogenetic chain of reactions. It consists in the occurrence of obstructive changes in the bronchial tract. As a rule, they affect the distal sections due to a sharp increase in the volume of mucus produced and developing bronchospasm.
Diagnosis of COPD: stages
It is customary to distinguish several stages.
The beginning of the pathology is zero. It is characterized by the production of sputum in large volumes, the person coughs regularly. Lung function at this stage of the disease is preserved.
The first stage is the period of development of the disease during which the patient chronically coughs. The lungs regularly produce large volumes of mucus. The examination reveals minor obstruction.
If a moderate form of the disease is diagnosed, it is distinguished by clinical symptoms (described earlier) that appear during physical activity.
A diagnosis of COPD, stage three, means it has become life-threatening. With this form of the disease, the so-called “pulmonary heart” appears. Obvious manifestations of the disease: restriction of air flow when exhaling, shortness of breath is frequent and severe. In some cases, bronchial obstruction is observed, which is typical for an extremely severe form of the pathology. This is dangerous for human life.
Not easy to identify
In fact, the diagnosis of COPD is made in the initial form of the disease much less often than it actually occurs. This is due to the fact that the symptoms are not clearly expressed. At the very beginning, pathology often flows secretly. The clinical picture can be seen when the condition progresses to moderate severity and the person consults a doctor complaining of sputum and cough.
At an early stage, there are often occasional cases when a person coughs up a large volume of sputum. Because it occurs infrequently, people rarely worry and do not seek medical attention in a timely manner. They come to the doctor later, when the progression of the disease leads to a chronic cough.
Definition of disease
Chronic obstructive pulmonary disease is a pathological inflammatory process in the lungs, the main consequence of which is the inability to breathe normally. A constant lack of oxygen in the body gradually leads not only to constant shortness of breath and painful coughing attacks. At the same time, physical activity decreases, since in the later stages even trying to climb a few steps on the stairs causes severe shortness of breath.
The insidiousness of the disease is that it can occur without a cough, which is why it is often diagnosed late.
The main symptoms of COPD are:
- Dry cough. In the early stages, it may not appear, which complicates the early diagnosis of the disease. But more often than not, a mild cough without sputum is not taken seriously, which is why a person seeks help from a doctor too late.
- Sputum. After some time, the cough becomes wet, with clear sputum being coughed up. In the later stages, the sputum becomes thick and abundantly secreted, often interspersed with pus.
- Dyspnea. Caused by a lack of oxygen in the body and a chronic inflammatory process in the lungs. Appears at the last stage of COPD development, when changes in lung tissue become irreversible. It is observed with significant physical exertion or the weakest acute respiratory viral infection.
In addition, the disease provokes increased secretion of mucus in the bronchi, pulmonary hypertension, gas exchange disorders, and hemoptysis.
Chronic obstructive pulmonary disease has the following main phases:
- First. The disease itself is mild, manifested only by rare bouts of coughing. At this stage, pathological changes in the lungs are almost invisible. At this stage, further development of the disease in some cases can be stopped with timely treatment.
- Second. In the second stage, people most often begin to seek medical help. The cause is sharply manifested symptoms, such as cough with sputum and incipient shortness of breath. Pathological changes in the lungs become irreversible. After this, treatment can only be aimed at slowing down the progression of the disease.
- Third. At the third, rather severe stage, the volume of air entering the lungs sharply decreases. This is associated with the development of obstructive phenomena, characterized by severe shortness of breath and coughing attacks with purulent sputum.
- Fourth. The most severe stage, which leads to complete loss of ability to work and poses a threat to life. It is at this stage that a pathology such as “cor pulmonale” appears and respiratory failure appears.
The development of chronic obstructive pulmonary disease is provoked by the following main factors:
- long-term smoking;
- polluted air in the house (for example, due to the use of solid fuel for heating);
- low socio-economic status of a person or his family;
- chronic infectious diseases of the lower respiratory tract (chronic obstructive bronchitis or bronchial asthma);
- adenoviral infection;
- deficiency of vitamin C in the body;
- conditions of professional activity associated with the presence of dust and chemical vapors in the air (varnishes, paints, gases).
Another common cause of COPD is the so-called passive smoking. That is why health problems arise not only for the smoker himself, but also for all members of his family. This is especially dangerous for children, as it increases the risk of developing COPD in the future.
Proper and timely treatment of lower respiratory tract diseases in childhood helps prevent the development of COPD in adulthood.
A dry cough with shortness of breath may be a symptom of chronic obstructive pulmonary disease.
The situation is getting more complicated
If the disease has been diagnosed and treatment measures have been taken, for example, traditional treatment for COPD does not always show good results. Often the complication occurs due to a third-party infection.
When additional infection occurs, even at rest the person suffers from shortness of breath. There is a change in the nature of the discharge: the sputum turns into purulent. There are two possible ways of developing the disease:
- bronchial;
- emphysematous.
In the first case, sputum is released in very large volumes and the cough is regularly tormented. There are frequent cases of intoxication, the bronchi suffer from purulent inflammation, and cyanosis of the skin is possible. The obstruction develops strongly. Pulmonary emphysema for this type of disease is characterized by mild.
With the emphysematous type, shortness of breath is fixed respiratory, that is, it is difficult to exhale. Pulmonary emphysema predominates. The skin takes on a pinkish gray tint. The shape of the chest changes: it resembles a barrel. If the disease follows this path, and also if the correct drugs for COPD have been chosen, the patient has a high probability of living to an old age.
Stability and instability in COPD
The disease can be in one of two forms: stable or acute. With a stable development, no changes in the body can be found when observing the dynamics of changes over weeks or months. You can notice a certain clinical picture if you regularly examine the patient for at least a year.
But with an exacerbation, just a day or two already shows a sharp deterioration in the condition. If such exacerbations occur twice a year or more often, they are considered clinically significant and may cause the patient to be hospitalized. The number of exacerbations directly affects the quality of life and its duration.
In special cases, patients are smokers who previously suffered from bronchial asthma. In this case, they talk about “cross syndrome”. The body tissues of such a patient are not able to consume the amount of oxygen necessary for normal functioning, which sharply reduces the body’s ability to adapt. In 2011, this type of disease was no longer officially classified as a separate class, but in practice, some doctors still use the old system today.
How will a doctor detect the disease?
When visiting a doctor, the patient will have to undergo a series of tests to determine COPD or find another cause of health problems. Diagnostic measures include:
- general examination;
- spirometry;
- a test through a bronchodilator, which includes inhalations for COPD, before and after which a special study of the respiratory system is carried out, observing changes in indicators;
- radiography, additionally - tomography, if the case is unclear (this allows you to assess how large the structural changes are).
Sputum samples must be collected for analysis of secretions. This allows us to draw conclusions about how severe the inflammation is and what its nature is. If we are talking about an exacerbation of COPD, then from the sputum we can draw conclusions about which microorganism provoked the infection, as well as what antibiotics can be used against it.
Body plethysmography is performed, during which it is assessed. This makes it possible to clarify lung volume, capacity, as well as a number of parameters that cannot be assessed with spirography.
Be sure to take blood for a general analysis. This makes it possible to identify hemoglobin and red blood cells, against the background of which conclusions are drawn about oxygen deficiency. If we are talking about an exacerbation, then a general analysis provides information about the inflammatory process. The number of leukocytes and ESR are analyzed.
The blood is also examined for gas content. This makes it possible to detect not only the concentration of oxygen, but also carbon dioxide. It is possible to correctly assess whether the blood is sufficiently saturated with oxygen.
Indispensable tests are ECG, ECHO-CG, ultrasound, during which the doctor receives correct information about the condition of the heart, and also finds out the pressure in the pulmonary artery.
Finally, fiberoptic bronchoscopy is performed. This is a type of study during which the condition of the mucous membrane inside the bronchi is clarified. Doctors, using special preparations, obtain tissue samples that allow them to study the cellular composition of the mucosa. If the diagnosis is unclear, this technology is indispensable for clarifying it, as it allows us to exclude other diseases with similar symptoms.
Depending on the specifics of the case, an additional visit to a pulmonologist may be prescribed to clarify the condition of the body.
Treatment of COPD with drugs (list of drugs)
The basis of drug treatment is various drugs that help expand the bronchi and relax their muscles. First of all, these are drugs from the group of bronchodilators (bronchodilators). At each stage of the development of the disease, its own groups of medications are used, the volume of use of which is increasing.
At the initial stage of the disease, the doctor prescribes drugs from the group of bronchodilators. Depending on the severity of the disease, they can be used constantly or on demand during an exacerbation. For this, the following list of medications is used:
- Anticholinergics;
- β2-adrenergic agonists;
- Theophylline.
Most often they are prescribed in a course of 10–14 days during an exacerbation period. For COPD, the preferred method of administering the drug is inhalation, using a modern nebulizer.
Additionally, antioxidants with a mucolytic effect are used. Most often, a drug such as N-acetylcysteine is used for this, used at a dosage of 600 milligrams per day. It can be used long-term, from 3 to 6 months, on an outpatient basis.
In more severe stages, long-acting bronchodilators used by inhalation become the main drugs. Most often, these are quite expensive drugs, most often used for treatment in a hospital setting. These may be combination drugs such as:
- Salbutamol (100/200 mg, 2 inhalations 2 times a day);
- Budesonide or Formoterol (160/4.5 mcg, 2 inhalations 2 times a day);
- Salmeterol (50 mcg, 1 inhalation 2 times a day).
They can be used both in a hospital setting and on an outpatient basis, under the constant supervision of a physician. At this stage, mucolytic drugs such as Ambroxol, Carbocisteine or various iodine preparations are used to facilitate coughing up sputum.
On third
Long-acting bronchodilators in combination with glucocorticosteroids also remain the basis of treatment. Treatment of COPD at this stage should be carried out. These drugs have a pronounced anti-inflammatory effect, and therefore are even more effective than for bronchial asthma. For this purpose, drugs such as Fluticasone propionate at a dosage of 1000 mcg/day can be used.
We treat without medications
Treatment of COPD is a complex process that requires an integrated approach. First of all, we will consider non-drug measures that are mandatory for the disease.
- completely stop smoking;
- balance your diet, include protein-rich foods;
- adjust physical activity, do not overexert;
- reduce weight to the standard if you have extra pounds;
- regularly walk slowly;
- go swimming;
- practice breathing exercises.
What if with medications?
Of course, you can’t do without drug therapy for COPD either. First of all, pay attention to vaccines against influenza and pneumococcus. It is best to get vaccinated in October-mid-November, since then the effectiveness decreases, the likelihood increases that there have already been contacts with bacteria and viruses, and the injection will not provide an immune response.
They also practice therapy, the main goal of which is to expand the bronchi and keep them in normal condition. To do this, they fight spasms and use measures that reduce the production of sputum. The following medications are useful here:
- theophyllines;
- beta-2 agonists;
- M-anticholinergics.
The listed drugs are divided into two subgroups:
- long-acting;
- short action.
The first group maintains the bronchi in normal condition for up to 24 hours, the second group lasts 4-6 hours.
Short-acting medications are relevant at the first stage, as well as in the future, if there is a short-term need for this, that is, symptoms suddenly appear that need to be urgently eliminated. But if such medications do not provide sufficient results, they resort to long-acting medications.
Also, anti-inflammatory drugs should not be neglected, as they prevent negative processes in the bronchial tree. But you also can’t use them outside of doctors’ recommendations. It is very important that the doctor supervise drug therapy.
The main components of COPD treatment
Drug therapy and pulmonary rehabilitation are the main components of COPD treatment worldwide.
Drug therapy is carried out to reduce the severity of symptoms, reduce the frequency and severity of exacerbations, prevent and treat complications, as well as increase tolerance to physical activity and improve quality of life.
What is pulmonary rehabilitation?
Pulmonary rehabilitation (respiratory rehabilitation) is an effective therapeutic strategy for reducing shortness of breath, improving health status and exercise capacity.
The main component of pulmonary rehabilitation programs is physical therapy, but psychological support and diet are also available.
What does physical therapy do?
The use of therapy (rehabilitation) programs using physical education is recommended at all stages of COPD. Physical therapy helps increase the strength of the respiratory muscles and muscles of the legs and arms, reduce chest tightness and shortness of breath, and improve physical condition.
It has been proven that physical education, as well as breathing exercises, helps reduce the number of exacerbations and the number of visits to medical help, improves endurance, increases tolerance to physical activity, and improves the quality of life.
Features of physical therapy for COPD
The minimum duration of an effective program of physical education and/or respiratory therapy for COPD should be at least 4 weeks, on average 8-12 weeks.
The positive effect after completing the therapy program persists for several months, although after stopping the exercises, the initial improvement in all parameters is gradually lost.
(Breathing exercises according to Strelnikova)
Where and when is therapy performed?
Once you have been diagnosed with COPD, you should consult with a physical therapist about ways to maintain your physical activity and breathing exercises.
The use of therapy during and after any exacerbation will help to quickly overcome it and prevent the development of possible complications, return to the usual rhythm of life, and restore performance. If treatment is carried out in a hospital, then physical therapy is carried out there and continues after discharge.
An important component of pulmonary rehabilitation is informing patients about the characteristics of the disease with which they will now live.
The main way to slow down COPD is to stop smoking!
It should be remembered that an increase or excessive decrease in body weight worsens your health and can lead to an increase in shortness of breath.
The following factors can cause deterioration in health:
- smoking,
- refusal or omission to take prescribed treatment,
- improper use of the inhaler,
- untreated concomitant diseases,
- lack of regular medical supervision,
- lack of physical therapy.
(Breathing exercises according to Strelnikova, with description)
Serious therapy is not a reason to be afraid
For COPD, glucocorticosteroid hormonal drugs are prescribed. Typically in the form of inhalations. But in tablet form, such drugs are good during an exacerbation. They are taken in courses if the disease is severe and has developed to a late stage. Practice shows that patients are afraid to use such remedies when the doctor recommends them. This comes with concerns about side effects.
You should remember that most often adverse reactions are caused by hormones taken in the form of tablets or injections. In this case, it is not uncommon:
- osteoporosis;
- hypertension;
- diabetes.
If the drugs are prescribed in the form of inhalations, their effect will be milder due to the small dose of the active substance entering the body. This form is applied topically, affecting primarily what and helps to avoid most side effects.
You also need to take into account that the disease is associated with chronic inflammatory processes, which means that only long courses of medications will be effective. To understand whether there is a result from the chosen drug, you will have to take it for at least three months, and then compare the results.
Inhalation forms may cause the following side effects:
- candidiasis;
- hoarse voice.
To avoid this, you need to rinse your mouth every time after taking the product.
Treatment of chronic obstructive pulmonary disease
The basic principles of therapy for COPD are:
- quitting smoking;
- timely initiation of drug treatment;
- development of a treatment regimen by the attending physician individually for each patient, taking into account the severity of his condition, the symptoms present and their intensity;
- vaccination of patients against influenza and pneumococcal infections (of course, only on a voluntary basis);
- physical activity to improve respiratory function (a daily 20-minute walk in the fresh air helps strengthen the lungs).
In severe cases of COPD and the development of respiratory failure, oxygen inhalation is prescribed.
To give up smoking
Quitting smoking is not as easy as it seems. Since COPD develops mainly in people who are heavy smokers, it will be very difficult for them to give up the bad habit. However, it is this step that gives hope for alleviating the symptoms of the disease and improving life prospects.
To speed up the process of quitting tobacco addiction, you can resort to the following measures:
- the use of skin patches used as nicotine replacement treatment;
- consultations with a narcologist, psychologist and other medical specialists;
- attending group programs and self-help sessions for smokers;
- the patient’s independent formation of a psychological attitude that smoking is harmful and dangerous to health and life.
Anti-tobacco programs help prolong the life of a COPD patient by an average of 1 year. Of course, they are not free, but they are very effective, as the practice of many developed European and non-European countries (Great Britain, USA) has shown.
Medicines
Pharmacotherapy has several goals:
- reduction in the intensity of COPD symptoms;
- inhibition of the progression of the pathological process;
- preventing frequent relapses of pathology.
The disease cannot be completely cured, but it is quite possible to alleviate its course with the help of certain medications. For this purpose, they resort to the following:
- bronchodilators;
- drugs based on corticosteroids;
- expectorants;
- phosphodiesterase-4 inhibitors;
- immunomodulators.
Each of the above groups of medications has its own mechanism of action and features of use. There can be no talk of any self-medication!
Bronchodilators
The mechanism of action of bronchodilators is to expand the bronchial lumen, thereby facilitating the movement of air through them during exhalation. In addition, this group of drugs significantly improves the tolerance of physical stress.
Bronchodilators are divided into several subgroups:
- Beta stimulants of short duration. These include the drugs Salbutamol, Ventolin, Fenoterol.
- Long-acting beta stimulants: Salmoterol, Formoterol.
- Short-term anticholinergics: Atrovent (ipratropium bromide).
- Anticholinergics with a prolonged effect: Spiriva (tiotropium bromide).
- Xanthines (Euphylline, Theophylline, Neophylline).
Most boncholytics are intended for inhalation administration. Moreover, they can be dispensed in different forms - inhalation powders, aerosols, inhalers that are activated during inhalation, nebulas with a solution for spraying through a nebulizer, etc. It is noteworthy that for seriously ill patients, as well as for patients with mental disorders, it is preferable to use liquid solutions for inhalation through a nebulizer.
Bronchodilators are the main component of therapy for COPD. They can be used either independently or as part of a complex treatment.
For continuous use, the second and fourth groups of bronchodilators are recommended, since they have a prolonged effect. If it is necessary to prescribe short-acting drugs, preference is given to the combination of fenoterol with ipratropium bromide (for example, Berodual).
Xanthines (Euphylline, Theophylline, Neophylline) are taken in tablet form. However, they can cause serious side effects, so their long-term use is not advisable.
Glucocorticosteroid hormones (GCS)
GCS are potent anti-inflammatory drugs. They are prescribed to patients with severe and extremely severe COPD, as well as during exacerbation of the disease, which occurs in a moderate degree.
It is best to use GCS in the form of inhalations (Budesonide, Beclomethasone, etc.). This use minimizes the incidence of systemic side effects, which often occur when taking hormonal drugs of this group orally.
GCS are practically not prescribed in isolation; it is preferable to combine them with beta-agonists. This combination is ideal for long-term treatment of COPD. List of the most frequently prescribed combined corticosteroids:
- Symbicort (active ingredients – formoterol and budesonide);
- Seretide (salmoterol and fluticasone).
In severe cases of COPD, systemic use of glucocorticosteroids - Prednisolone, Dexamethasone, Kenalog - may be required. However, their prolonged use threatens the development of serious side effects that can manifest themselves in the form of erosive and ulcerative lesions of the gastrointestinal tract, the development of Itsenko-Cushing syndrome, steroid diabetes, bone osteoporosis, etc.
It is important to consider that although bronchodilators are the mainstay of treatment for COPD, they can lead to serious illnesses, therefore, a treatment regimen, including the prescription of specific medications, their dosage and the duration of their course of use, is developed only by the attending physician individually for each patient.
Other drugs
If there are difficulties with coughing and removing sputum, mucolytics are prescribed. One of the most effective is the drug Daxas.
This is a relatively new drug belonging to the group of phosphodiesterase-4 inhibitors. It has a long-lasting anti-inflammatory effect and can be prescribed as an alternative to GCS. Available in tablet form.
Take 1 tablet (500 mg) 1 time per day for severe and extremely severe COPD. However, the drug has its drawbacks, the main ones being high cost and high risks of side effects (nausea, vomiting, dizziness, etc.).
The drug Erespal also has a pronounced anti-inflammatory effect, so it can also be used to alleviate the condition of a patient with COPD.
In parallel with pharmacotherapy, a course of physiotherapy is carried out. In particular, intrapulmonary percussion ventilation is a manipulation during which small streams of air are generated that enter the lungs with the help of quick pushes. They are created by a special medical device.
What else will help?
For COPD, antioxidant drugs containing a complex of vitamins A, C, and E are actively used. Mucolytic agents have proven themselves well, as they dilute the sputum produced by the mucous membrane and help cough it up. In case of severe development of the situation, artificial ventilation of the pulmonary system is useful. If the disease worsens, you can take antibiotics, but under the supervision of a doctor.
Selective phosphodiesterase-4 inhibitors have brought considerable benefit. These are quite specific drugs that can be combined with some drugs used in the treatment of COPD.
If the disease is caused by a genetic defect, then it is customary to resort to replacement therapy. For this purpose, alpha-1-antitrypsin is used, which, due to a congenital defect, is not produced sufficiently by the body.
Treatment of the disease
How to treat COPD? Obstructive pulmonary disease is incurable, but if no treatment is applied, the disease will progress rapidly, causing severe pain while breathing.
The first thing to do to stop the development of the disease is to get rid of the habit of consuming nicotine, even if the lungs have been affected by the disease for a very long time.
Medicines prescribed by a doctor are necessary to improve the respiratory process.
Medicines intended to treat COPD include drugs such as bronchodilators (fenoterol, salbutamol), designed to widen the bronchi by relaxing the muscles in their walls. In addition, therapy with mucolytic drugs is prescribed, among which are bromhexine and ambroxol, they dilute the mucus, helping it leave the respiratory tract.
Treatment also requires antibiotics used during an exacerbation. Inhibitor drugs prevent the inflammatory process from spreading, and glucocorticosteroids and hormonal agents are also useful for exacerbations and obvious respiratory failure.
Currently, inhalations are considered one of the most effective and safe ways to treat respiratory diseases. Inhalation helps the medicine get directly into the lungs, but inhalation should only be done with a doctor's prescription. Inhalation is carried out with a nebulizer, and doctors are resorting to such treatment more and more often.
Preventive measures
What is the practice for preventing COPD? Are there effective ways to prevent the development of the disease? Modern medicine says that it is possible to prevent disease, but for this a person must take care of his health and treat himself responsibly.
First of all, you need to stop smoking, and also about the possibility of avoiding being in harmful conditions.
If the disease has already been detected, its progression can be slowed by applying secondary preventive measures. The most effective ones were:
- vaccination to prevent influenza and pneumococcus;
- Regularly taking medications prescribed by your doctor. Remember that the disease is chronic, so temporary therapy will not bring real benefit;
- control over physical activity. This helps train the muscles of the respiratory system. You should walk and swim more, use breathing exercises;
- inhalers. They need to be able to use correctly, since incorrect use leads to the absence of results from such therapy. As a rule, the doctor is able to explain to the patient how to use the medication so that it is effective.
It must be emphasized that chronic obstructive pulmonary disease is a disease that “grows” on the “foundation” of chronic bronchitis. Therefore, these diseases will have common diagnostic criteria given in the section “Chronic bronchitis”. Additional diagnostic criteria for chronic obstructive pulmonary disease are signs of bronchial obstruction, which in this disease is permanent and not completely reversible, as well as pulmonary emphysema. The leading place in the diagnosis of bronchial obstruction is occupied by the study of external respiration function with bronchodilation tests. For this purpose, modern spirographic devices (such as MasterScop, Spiroset) are used, which record the “flow-volume” curve of a forced breathing maneuver and carry out computer processing of the obtained data. The most informative and accessible indicators for assessing the degree of bronchial obstruction in COPD are FEV1 and the FEV1/FVC ratio (Tiffno index). The diagnostic criterion for chronic obstructive pulmonary disease is a decrease in FEV1 of 80% of the required values, indicating the initial manifestations of bronchial obstruction. It should also be taken into account that in severe cases of chronic obstructive pulmonary disease in stages III-IV of the disease, a significant decrease in FVC occurs in parallel with a decrease in FEV1. Therefore, in these cases, the FEV1/FVC indicator loses its diagnostic value. To clarify how quickly COPD progresses, FEV1 is monitored for at least four years due to the fact that the individual test error is 5%. Many studies show that FEV1 in healthy smokers aged 30-40 years decreases by 20-30 ml per year. In most patients with chronic obstructive pulmonary disease, the annual decrease in FEV1 exceeds 30 ml and is more significant - from 45 to 90 ml. To clarify the level of bronchial obstruction, the maximum indicators of the expiratory flow rate are calculated at the level of 75%, 50% and 25% of FVC remaining in the lungs at the time of measurement - the maximum volumetric flow rates MOS75 = FEF25, MOS50 = FEF50, MOS25 = FEF75 and the average volumetric flow rate in the range 25%-75% FVC - SOS25-75 - Bronchial obstruction at the level of small bronchi is manifested, first of all, by a decrease in MOS25 (FEF75) and to a lesser extent - SOS25-75 (see Fig. 6). To determine the reversibility of bronchial obstruction, tests are used with bronchodilators - short-acting β2-agonists salbutamol and fenoterol.
Rice. 6. Flow-volume curve of patient B., 41 years old. Signs of pulmonary insufficiency of the obstructive type with significant impairment of bronchial patency at all levels. FEV1 - 55.3% of the expected value, Tiffno index - 61.8%
The use of tests with bronchodilators largely characterizes the possibility of reversibility of bronchial obstruction. An increase during the FEV1 test by more than 15% of the initial values is conventionally characterized as reversible obstruction. It is generally accepted that an improvement in FEV1 of less than 15% after inhalation of a short-acting bronchodilator is more in favor of the diagnosis of COPD (Fig. 7). In some cases, even a deterioration of the analyzed indicator is determined. This indicates incomplete reversibility or irreversibility of bronchial obstruction. On the contrary, reversible bronchial obstruction with an increase in FEV1 by more than 15% of the initial value after inhalation of a bronchodilator is characteristic of bronchial asthma.
Rice. 7. Flow-volume curve of patient K., 62 years old. Moderate impairment of the ventilation function of the lungs of a mixed type with a significant impairment of bronchial obstruction at the level of the middle and small bronchi. Bronchodilation test with fenoterol/ipratropium bromide is negative. Increase in FEV1 - 9%
At home, to monitor the degree of bronchial obstruction and control the effectiveness of treatment, the POSV indicator is used, which is recorded using a home peak flow meter by the patient himself, who is properly trained. Peak flowmetry makes it possible to easily measure daily fluctuations (variability) of bronchial obstruction, which in COPD usually does not exceed 15%. At the same time, with progressive pulmonary emphysema, one cannot focus only on the peak expiratory flow rate. This indicator can be only moderately reduced and does not characterize the true magnitude of pulmonary insufficiency. In these cases, the results of measuring FEV1 when recording the forced expiratory flow-volume curve show a more significant decrease in the indicator, corresponding to the degree of ventilation failure.
Measurement of arterial blood gas composition is recommended for stages III and IV COPD. A study of blood gas composition is necessary to assess pulmonary gas exchange, determine the nature of disease progression and the degree of pulmonary insufficiency, as well as the timely administration of long-term oxygen therapy.
Chronic obstructive pulmonary disease (COPD diagnosis) is a pathological process characterized by partial restriction of air flow in the respiratory tract. The disease causes irreversible changes in the human body, so there is a great threat to life if treatment is not prescribed on time.
How to cure COPD
Chronic obstructive pulmonary disease (COPD for short) is a lung disease in which the airflow into the lungs is limited due to inflammation of the lung tissue.
Not knowing how to cure COPD, the patient constantly feels shortness of breath, lack of respiratory function, coughs and cannot completely cough, although the cough is productive (sputum is produced).
He cannot perform physical activity because the respiratory system is not able to satisfy the body's increased need for oxygen.
We will tell you:
The disease is steadily progressing, therefore, if the patient does not take any action to get rid of COPD, death is not long in coming. Almost always, the disease leads to partial and then complete loss of ability to work, and in some cases to disability.
How dangerous is COPD if left untreated?
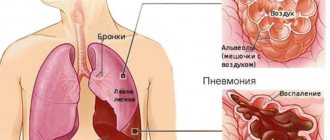
COPD is caused by exposure to negative environmental factors (most often cigarette smoke, industrial emissions). In response to toxins and irritants coming from the inhaled air, the functions of the secretory apparatus change. Mucus begins to be released in large quantities, its properties change. The tissues of the lungs and bronchi become inflamed and become vulnerable to various types of infections.
Two negative processes are observed simultaneously: constant swelling and narrowing of the airways in combination with deformation of the lung tissue, loss of its function, and the release of excess mucus. As a result, reactions develop that lead to damage to the bronchi, bronchioles and alveoli.
Associated symptoms of COPD are:
- weight loss,
- pulmonary hypertension,
- formation of the “pulmonary heart”,
- osteoporosis,
- anxiety disorders,
- gastroesophageal reflux.
COPD is diagnosed on the basis of chest X-ray, pulmonary function tests, and the presence of characteristic systemic diseases that contribute to its development - dependence on intravenous drugs, bronchiolitis, eosinophilic granuloma, HIV infection.
How to treat COPD in adults
When telling patients how to treat COPD in adults, doctors first mention bronchodilators. These are drugs, under the influence of which the smooth muscles of the walls of the bronchi relax, due to which the bronchi expand.
To the question whether COPD can be cured, modern medicine gives a negative answer. The proposed traditional methods, which are based on pharmacotherapy, make it possible to prevent deterioration of the condition and improve the quality of life. They cannot completely eliminate existing violations.
The patient can cough up mucus easily. Stagnation of mucus in the lungs is fraught with inflammation. Main types of bronchodilators:
- M-anticholinergics, for example, Spiriva, Atrovent;
- long-acting beta-two agonists, for example, Formoterol, Salmeterol.
The list of drugs that are used in the treatment of COPD also includes:
- glucocorticosteroids . As a rule, they are prescribed in cases of acute respiratory failure. Local or systemic drugs are used. Prednisolone is most often used in tablets or in the form of intravenous infusion. When the patient's condition has stabilized, he should be transferred to inhaled forms of steroid hormones.
- antibiotics _ Drugs of this class are also used during exacerbation of the disease. The fact is that as a result of the destruction of bronchioles, emphysema occurs, which impedes the outflow of mucus. The accumulation of mucus is a favorable environment for the development of bacteria that cause bronchitis and pneumonia. To avoid them, patients are prescribed drugs belonging to the second generation of cephalosporins, fluoroquinolones, and other drugs that act primarily on the bronchial flora. Antibiotics can be administered by inhalation (nebulizer therapy), intramuscularly, intravenously or orally. Bronchial infection is diagnosed by the presence of yellow or green sputum. In a hospital setting, patients undergo bacterial cultures.
- mucolytics . These drugs thin the mucus and facilitate its removal from the bronchi. As a result, bacteria do not have time to accumulate in quantities sufficient to develop bronchitis or pneumonia. They are divided into drugs of direct and indirect action.
- indirect-acting drugs affect the secretion of mucus in the respiratory tract. At the same time, they do not affect the mucus that has already been released. The most common are Bromhexine and Ambroxol.
- Direct acting drugs act directly on the mucus that is already in the bronchi. When in contact with mucus, the enzymes in their composition dilute it and contribute to the loss of its adhesive properties. They are administered primarily by inhalation. The most common are Chymotrypsin, Trypsin.
- other drugs . To replace glucocorticosteroids, which have a number of side effects (especially when used systemically), drugs are taken that neutralize the effect of inflammatory mediators or receptors sensitive to them, for example, Fenspiride.
During the complex treatment of COPD, doctors also pay attention to the treatment of concomitant diseases, for example, cor pulmonale.
Quitting smoking, stopping contact with harmful production factors (transferring to another job), and moving to an ecologically clean area are of decisive importance.
The patient’s contact with solid fuel combustion products (coal, firewood) and other irritants should be limited.
How it works?
Neurodoctor affects the control centers of the brain.
The brain begins to produce dozens of neurohormones and form “corrective” nerve impulses.
Neurohormones are many times more effective than the most powerful drugs in quickly curing the disease. Nerve impulses eliminate pathological processes at the cellular level and correct the functioning of other organs and systems of the body.
LEARN MORE ABOUT THE METHOD
In some cases, doctors have to use surgical techniques to treat COPD.
Most often, surgeons remove large bullae of pulmonary tissue, which cause hemoptysis, severe shortness of breath, and are sites of systematic infections. In some cases, a lung transplant is performed.
These operations carry significant risks, with a 10 to 15% chance of death.
How to cure COPD forever at home?
In recent years, technology has emerged that gives a positive answer to the question of how to cure COPD forever. This is color pulse stimulation of body cells, which triggers a self-healing mechanism.
Since all processes occurring in organisms occur under the guidance of the brain, the device primarily affects brain cells. This is done through light pulses that have a predetermined polarity, frequency and sequence.
Correction of the control structures of the brain stimulates the production of neurohormones, which affect the body much more efficiently and stronger than pharmaceutical drugs and have no side effects.
Under the influence of "Neurodoctor"
- degeneration of lung tissue slows down,
- the inflammatory reaction stops,
- mucus production returns to normal.
When starting to use the device, you should not abruptly refuse medications prescribed by your doctor. The transition to a “pill-free life” should occur gradually and under the supervision of a doctor. About 67% of patients note a significant improvement in their well-being after just a few sessions of using the device.
To obtain a lasting result, you should complete the full course of treatment. The result is guaranteed. If the patient doesn’t like something, he can return Neurodoctor within a month from the date of purchase and get 100% of the money paid back.
How to treat COPD at home is no longer a question, because the device is designed for home use.
Order Neurodoctor and be healthy!
Source: https://www.avatar-medical.ru/diseases/pulmonology/hobl/